Suspected arrhythmia clinic referral form VISION

Refer patients with red flag signs to
A&E
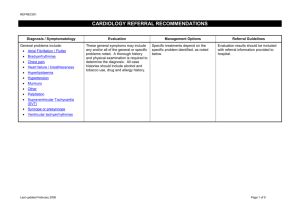
Referral criteria for
Community Clinic
Manage in Primary
Care
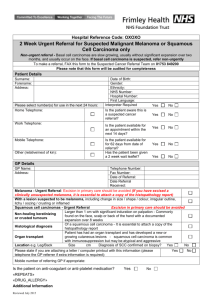
Suspected Arrhythmia Clinic Referral Form
Complete and fax form to 0208 401 3022 ,
Telehpone Enquiries 0208 401 3000 ext. 5771, Bleep 273
Consider using Cardiology advice service
Patient acutely unwell, haemodynamic compromise, heart failure
High-grade (2 nd or 3 rd degree) heart block, except nocturnal Wenkebach
Ventricular tachycardia
Exercise-induced syncope
Syncope associated with angina or known structural heart disease (e.g. previous MI, valvular heart disease, cardiomyopathy, left ventricular hypertrophy)
Syncope with abnormal ECG e.g. evidence of acute ischaemia or prior MI, left ventricular hypertrophy, long QT, LBBB
Symptomatic bradycardia
Recurrent dizziness or syncope
Recurrent palpitations
New diagnosis “Supra-ventricular tachycardia” (SVT)
New diagnosis atrial fibrillation or flutter, unless patient is asymptomatic and >65yrs old
Patients with known arrhythmia already under Cardiologist follow-up will be re-directed to Cardiology
OPC
Single episode of palpitation or dizziness, or
Suspected vasovagal syndrome responding to simple conservative measures
AND no evidence of structural heart disease
(i.e. normal 12-lead ECG, normal physical examination, normal echocardiogram)
First name:* «PATIENT_Forename1»
Address:* «PATIENT_BlockAddress»
Patient Details
Last name:* «PATIENT_Surname»
DOB:* «PATIENT_Date_of_Birth»
NHS number:* «PATIENT_New_Format_NHS_Number»
Ethnicity:
GP Details
GP Name: «REFERRAL_Clinician»
Practice Name and Address: «PRACTICE_Name»
«PRACTICE_BlockAddress»
Phone:* «PATIENT_Main_Comm_No»
«PATIENT_Mobile_No»
Interpreter:
Referral Details
Date of referral:*
«REFERRAL_Event_Date»
Suspected Arryhthmia Clinic Referral Form
Clinical History
Palpitations (specify frequency
Syncope
Shortness of breath
Dizziness Fatigue
Asymptomatic (incidental finding) Other (please specify)
Reason for referral
Syncope / dizziness AF/flutter
Past Medical History and Co-morbidities (please tick)
Palpitations Other
IHD Alcohol intake
AF Renal Failure
Hypertension Valvular Heart Disease
Lung disease Other
Clinical examination & Investigation (write in or attach results)
* = Essential information
Pulse* Blood Pressure*
Creat* TFT
Heart murmur*
12-lead ECG report attached*
Hb*
CXR requested
Echo report Holter monitor
Medications
If AF or flutter
Is anticoagulation indicated
Is there a contra-indication to anti-coagulation
«DRUG_ALLERGY» «REPEATS»
Initial Primary Care Management
Lifestyle advice – alcohol intake, work/life stress management, healthy eating, physical exercise, referral for psychological or psychiatric help where appropriate
Consider referral to weight management service.
Treat aggravating medical conditions e.g. thyrotoxicosis, anaemia
If atrial fibrillation or flutter, consider starting:
Beta blocker or rate-limiting calcium antagonist to treat tachycardia
Anti-coagulation to prevent stroke ( weblink arrhythmia alliance CHADS-Vasc )
Where would your patient prefer to be seen (1 st and 2 nd preferences)?
Croydon University Hospital
Purley War Memorial Hospital
Other hospital (please specify)
Earliest available appointment, no preference re: location
To be completed by clinic staff
Date referral received:
Suspected Arryhthmia Clinic Referral Form
ECG included?
Provisional appointment date:
Tests required before clinic appointment:
If inappropriate referral, referrer informed? Y/N
Date informed: Person informed: