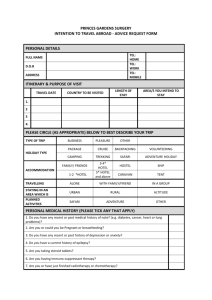
Travel Risk assessment form
advertisement

2016 ST JAMES’S TRAVEL RISK ASSESSEMENT FORM-patient to complete PATIENT TO COMPLETE 4-5 WEEKS PRIOR TO TRAVEL Please be aware that whilst we will try our best, it may not always be possible to accommodate your travel needs if you have short notice travel plans and we have limited appointments. NAME: DOB: Email: Telephone: Date of departure: Mobile: Total length of trip: Country to be visited: 1. M/F Exact location or region: City/rural Length of stay: 2. 3. Type of travel and purpose of trip – please tick all that apply holiday hotel backpacking business Expatriate cruise Safari Adventure Camping/hostels Volunteer work Pilgrimage Healthcare work Medical tourism Visiting family Diving Travel insurance? Y/N Do you plan to travel abroad again in the future? Please supply details of your medical history Y N Details Are you fit and well today Allergies – including food, latex, medication Severe reaction to previous vaccination Past operations, inc. removal of spleen and thymus gland Recent chemotherapy/radiotherapy/transplant Immune system condition Mental health inc. anxiety and depression Pregnant or breast feeding Current medication Please supply any records of vaccinations/malarial tablets that you may have had previously. 2016 Travel risk assessment form – to be completed by health professional Health Professional use only in conjunction with Travel Risk Assessment Form Patient Name: DOB: Travel risk management performed by: name&date Disease protection advised BCG/Mantoux Cholera Yes DT/IPV Hep A Hep B Hep A&B Hep A&typhoid Jap B Disease protection advised Influenza Meningitis ACWY MMR Rabies TBE Typhoid Yellow Fever Other Yes Malaria chemoprophylaxis recommendation Atovaquone/proguanil Chloroquine only Yes/ Discuss Choloroquine&proguanil Doxcycline Mefloquine Proguanil Weight of child Authorisation for a Patient Specific Direction (PSD) Following the completion of a travel risk assessment, the below named vaccines may be administered under this PSD to : NAME: DOB: Vaccine name Dose & schedule Prescriber: signature & date To discuss St James’s surgery travel advice leaflet given: Y/N (all topics below in patient information leaflet). Patient advised to read leaflet due to insufficient time to advise verbally during consult on every topic. Items ticked below indicate topics discussed specifically during the consultation: Prevention of accident&insurance advice Mosquito& insect bite prevention Food and water borne risks Malaria prevention advice Sexual health&blood borne virus risk Sun& heat advice Rabies specific advice Travellers’ diarrhoea advice