Travel questionnaire and info
advertisement

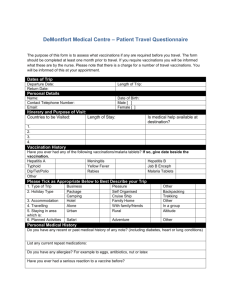
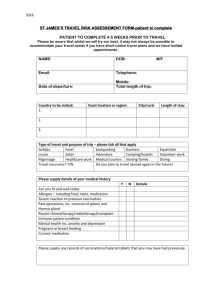
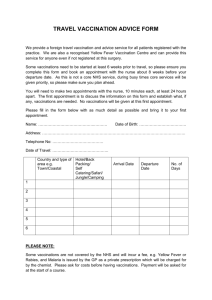
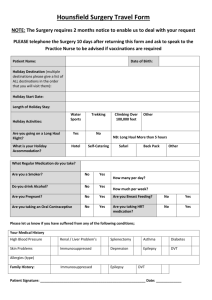
Torkard Hill Medical centre Travel health advice and vaccinations For advice on Travel, please contact the reception on 0115 963 3676 When planning your holiday it is important that you have accurate up-to-date advice about what immunisations and antimalarial protection you might need. Providing travel advice is a core part of the role of our experienced Practice Nursing team Prior to booking a nurse travel appointment, you will need to complete a Travel Clinic Questionnaire which can be downloaded here (insert hyperlink) or collected from reception. One of Practice Nurses will then contact you within 7 days of receipt of your form to arrange a convenient appointment. If you are advised that you need the following vaccinations, these are available free of charge from the Practice: Hepatitis A Typhoid Tetanus Diptheria Polio The NHS does not cover the cost of other travel vaccinations, such as Rabies, Yellow Fever, Hepatitis B, Japanese encephalitis, and Anti-malarial tablets. You will incur a charge if you require these vaccinations for your travel. We would like to remind all our patients that many travel vaccines and medications take several weeks to provide protection. It is vital therefore that you book your consultation in sufficient time before your holiday. Ideally, please contact the Practice 6-8 weeks in advance of travel. The practice does not provide a service for last-minute travellers, if you need urgent travel advice contact Travel doc at Regent Street Freephone 0800 583 3331 or The Walk-in Centre on London Road, Nottingham telephone: 0115 8838500. For further information about countries and required vaccinations, please see the links below. Links to websites on travel health: Travel Health www.travelhealth.co.uk Fit for Travel www.fitfortravel.scot.nhs.uk Foreign and Commonwealth Office www.fco.gov.uk/en/travel-and-living-abroad/ Travewww.traveldoctor.co.uk Torkard Hill Medical Centre Travel Vaccination Questionnaire One form per person travelling. Traveller to complete. Name of Traveller: Date of Birth: Travel Itinerary Date of Departure: Destinations(s) & duration of stay in each place: Type of Holiday (delete as applicable): Holiday / Businesss / VFR / Other (please state): Accommodation (delete as applicable): Hotel / Hostel / Family home / Other (please state): Any High Risk Activities Planned: (eg. Back packing, snorkelling, safari) Please state: Medical History Past/Current Medical History: Allergies: (Food, Drugs, Animals, Plants) Are you taking steroids: Do you have HIV: Are you pregnant: Are you planning pregnancy: Are you taking the contraceptive pill: Have you had ANY previous reactions to any vaccinations: Yes Yes Yes Yes Yes Yes / / / / / / No No No No No No Previous Vaccination Hisotry (if known) Vaccination Tetanus Diptheria Polio Date Typhoid Hep A Hep B Other All the information given is correct and up to date: Signed: Date: Please note: *Please return the completed form to the surgery at least 6 weeks before your departure date and the nurse will contact you to arrange an appointment. FOR PRACTICE NURSE USE ONLY: Vaccine Tick if BN & Expiry Date required Date Given Injection Site Signed Hep A Hep B Hep A & B Hep A with Typhoid Dip / Tet/ Polio Typhoid Meningitis Name of Prescribing Practitioner: Date: Signature: Malaria Tablets: Tablets Mefloquine Doxycycline Atovaquone plus Proguanil Chloroquine Proguanil Recommended Chosen Number Required Child Weight: Recommended Anti-Malarial Dose: Additional Comments: Travel Record Card Given: Yes / No / Updated Appointment Date & Time: Appointment with: Signed (Practice Nurse):