TB/LTBI Clinic Flow Sheet for Correctional Facilities
advertisement

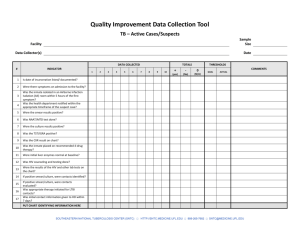
INMATE NAME ID # DOB TB/LTBI Clinic Flow Sheet for Correctional Facilities NAME OF PERSON COMPLETING THIS FORM: TITLE: ______________ NAME OF HEALTH DEPARTMENT STAFF ASSIST: TITLE: ______________ INMATE AKA AKA DOB INMATE ADDRESS CITY/STATE/ZIP EMERGENCY CONTACT NAME PHONE RECORD SEARCH INFORMATION SENT TO DATE FAX # PREVIOUS TX YEAR WHERE DATE READ DATE DATE CLASS TST ADMIN CHEST X-RAY Yes No Normal Abnormal CONFIRMED TX TREATMENT NO MEDICATIONS ORDERED MEDICATIONS ORDERED Start Date _____________________________ INH MG DAILY X MONTHS DOSES B6 MG DAILY X MONTHS DOSES EMB MG DAILY X MONTHS DOSES Rifampin MG DAILY X MONTHS DOSES Rifamate MG DAILY X MONTHS DOSES Other Medications (Please List) ______________________________________________________________________ LABS ORDERED/SPUTUMS/EDUCATION LABS ORDERED CMP CBC HIV LFTs SPUTUM SAMPLES EDUCATION PROVIDED HEPATITIS SCREEN MONTHLY URIC ACID OTHER MONTHS #1 COLLECTED – DATE #2 COLLECTED – DATE #1 RESULTS #2 RESULTS #3 COLLECTED – DATE #3 RESULTS ___________________ MEDICATION AUTHORIZATION SIGNED SOUTHEASTERN NATIONAL TUBERCULOSIS CENTER (SNTC) HTTP://SNTC.MEDICINE.UFL.EDU 888-265-7682 SNTC@MEDICINE.UFL.EDU CLINIC VISITS BASELINE Month 1 Month 2 Month 3 Month 4 Month 5 Month 6 Month 7 Month 8 Month 9 ALL MEDICATIONS MUST BE BY DIRECTLY OBSERVED - SWALLOWING (DOT) MEDICATIONS # DOSE INH B6 EMB RIF B/P PULSE TEMP URINE SKIN ASSESSMENT ABDOMEN COUGH NIGHT SWEATS RASH NEUROPATHY OTHER (describe) VISION COLOR HEARING SPUTUM WBC Hgb PLATELETS LABS AST ALT URIC ACID HIV HEPATITIS A HEPATITIS B HEPATITIS C Clinician’s Initials DATE TREATMENT COMPLETED TREATMENT NOT COMPLETED – REASON DATE RELEASED FROM FACILITY? NUMBER OF DOSES Refuses Medication RELEASE PLAN INITIATED Yes Other DISPOSITION COMMENTS CONFIDENTIAL MEDICAL RECORDS - Upon release or treatment completion, send record to this health department: ________________________ SOUTHEASTERN NATIONAL TUBERCULOSIS CENTER (SNTC) HTTP://SNTC.MEDICINE.UFL.EDU 888-265-7682 SNTC@MEDICINE.UFL.EDU No