intake form
advertisement

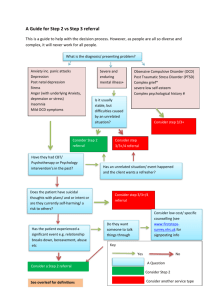
CLIENT INTAKE Personal Information Full Name: ____________________________________________________ Date:__________ I prefer to be called: ___________________________________ Age: ______ D.O.B.:________ Residential Address:_____________________________________________________________ ______________________________________________________________________________ Please list all of the phone numbers where we may call you: Home Phone: ______________________ May we leave a message? Yes/No Cell Phone: ________________________ May we leave a message? Yes/No Work Phone: _______________________ May we leave a message? Yes/No E-mail: ________________________ May we send you occasional e-mails regarding articles, books, resources, and events which may benefit you? (You can unsubscribe at any time) ? Y/N Referred by?: __________________________________________________________________ In case of emergency, please notify: Name: __________________________________________ Phone: _________________ Relationship:___________________________________________ Marital Status: ___ Never Married ___ Domestic Partnership ___Married ___Separated ___Divorced ___ Widowed Are you currently in a romantic relationship: ___Yes ___No Previous marriages/long-term partnerships: Length(s) of relationship(s): ____________________________ When ended: _______________ Reason: (widowed, divorced, etc.) __________________________________________________ Education School has been: ___ Easy ___ Fairly Easy ___ Difficult ___ Very Difficult Areas of achievement: ___________________________________________________________ Specific area(s) of difficulty: _______________________________________________________ Occupation Are you currently employed? ___ Yes __ No If yes, what is your current occupation? _____________________________________________ Do you enjoy your work? ___ Yes ___ No Please list any work-related stressors, if applicable: ____________________________________ ______________________________________________________________________________ Has your employer/supervisor ever expressed any of these concerns? (Check all that apply) ___ Missing too much work ___ Late too often ___ Increased errors ___ Irresponsibility ___ Poor/bad attitude ___ Difficulty getting along with other workers/supervisors Other_________________________________________________________________________ Health Physical Condition: ___ Excellent ___ Good ___ Fair ___ Poor Do you have a physical fitness program? ___ Not at all ___ Occasionally ___ Regularly Please list any significant illnesses, including allergies: ____________________________ Have you experienced any significant weight change in the last 2 months? ___ Yes ___ No If yes, please specify: _________________________________________________________ Are you having any difficulty with appetite or eating habits? ___ Yes ___ No If yes, please check where applicable: ___ Eating Less ___ Eating More ___ Bingeing ___Restricting ___ Purging Other: ________________________________________________ Are you having any problems with your sleep habits? ___ Yes ___ No If yes, check where applicable: ___ Difficulty falling asleep___ Insomnia ___ Sleeping too much ___ Poor Quality Sleep ___ Early morning waking ___ Disturbing dreams ___ Night terrors Please list any prescription and over-the-counter medications/supplements, including dosages if known: ______________________________________________________________________ ______________________________________________________________________________ Please list any persistent physical symptoms or health concerns: (e.g. chronic pain, headaches, hypertension, diabetes, etc.)______________________________________________________ Do you have any current or past history of addictive behavior? (e.g. drinking, drugs, gambling, etc.)__________________________________________________________________________ Do you drink alcohol? ___ Yes ___ No If yes, how much? ______________________________ Do you use other substances? ___ Yes ___ No If yes, which substances/how much? ________ ______________________________________________________________________________ Have you ever received treatment for alcohol/drug use? ____ Yes ___ No Please specify: ____ ______________________________________________________________________________ Do you now or have you ever attended a 12 step group? (AA, NA, ALANON, GA, etc.) ___ Yes ___ No If yes, please specify: ____________________________________________________ Are you currently experiencing anxiety, panic attacks or have any phobias? If yes, please elaborate, including when you began to experience these symptoms. _____________________ ______________________________________________________________________________ Are you currently receiving psychiatric services, professional counseling, or psychotherapy elsewhere? ___ Yes ___ No If yes, please specify: ____________________________________ Counseling History: ___ No previous treatment ___ Previous outpatient treatment ___ Previous Hospitalization Are you currently experiencing overwhelming sadness, grief, or depression? If yes, for approximately how long? _________________________________________________________ What significant life changes or stressful events have you experienced recently? ____________ ______________________________________________________________________________ What significant life changes or stressful events have you experienced in the past? __________ What is your current level of stress? ________________________________________________ Do you experience severe emotional and mood changes to the point where they make it difficult to function at your normal level? ___ Never ___ Seldom ___ Often Check which kind(s): ___ Anxiety ___ Manic states ___ Anger ___ Depression Have you ever had suicidal thoughts? ___ Never ___ Seldom ___ Often Have you ever attempted suicide? ___ Yes ___ No If yes, please explain: ___________________ ______________________________________________________________________________ Do you have any history of self-harm? ___ Yes ___ No If yes, please describe: ______________ ______________________________________________________________________________ How satisfied are you with your friendships and sense of support from others? _____________ ______________________________________________________________________________ What hobbies or interests do you enjoy? ____________________________________________ What do you consider some of your strengths? _______________________________________ What do you consider some of your weaknesses? _____________________________________ What do you like most about yourself? ______________________________________________ What do you like least about yourself? ______________________________________________ Do you consider yourself to be spiritual or religious? ___ Yes ___ No If yes, please describe your faith or belief system: _______________________________________________________ Do you have a system of saving money? ___ Yes ___ No Are you currently, or have you ever been, in a financial crisis? ___ Yes ___ No If yes, please specify: _______________________________________________________________________ Please list your reasons for counseling at this time: ____________________________________ ______________________________________________________________________________ What do you hope to accomplish in therapy? _________________________________________ ______________________________________________________________________________ What do you want to change about yourself in counseling? _____________________________ Family History Mother: Name_______________________________ Age_____ (If deceased, when?)________ Nationality_________________________ Highest level of education______________________ Occupation____________________ Abilities/special interests____________________________ General Health Status: Physical___________________ Emotional_________________________ Describe your relationship with her: ________________________________________________ Father: Name_______________________________ Age_____ (If deceased, when?)_________ Nationality: ___________________________Highest level of education____________________ Occupation: ___________________________ Abilities/special interests____________________ General Health Status: Physical ____________________Emotional:_______________________ Describe your relationship with him:________________________________________________ Number of Brothers: ______ Number of Sisters: ______ Name/Age/Occupation ___________ ______________________________________________________________________________ ______________________________________________________________________________ With whom did you live during your childhood? (Check all that apply) ___Mother & Father ___ Mother only ___ Father only ___ Mother & Stepfather ___ Father & Stepmother ___ Relatives ___ Foster Parents Other_____________________ Describe your childhood (infancy through age 12): ___ Very Happy ___ Pleasant ___ Bearable ___ Unhappy Please explain: _________________________________________________________________ ______________________________________________________________________________ Describe your adolescence (ages 12 through 21): ___ Happy ___Unhappy ___ Mixed Please explain: ________________________________________________________________ _____________________________________________________________________________ Check all that apply: ___I was not abused as a child ___I witnessed abuse in the home ___I was emotionally abused ___I was physically abused ___I was sexually abused as a child Please explain: ______________________________________________________________________________ ______________________________________________________________________________ Any family history of alcohol and/or drug abuse: ____ Who? ___________________________ Have any of your family members ever received counseling? ___ yes ___no If yes, who and for what reason?________________________________________________________________ ______________________________________________________________________________ Growing up in your family, were there any major crisis events: sicknesses; deaths; relocations; traumas; shameful happenings? Briefly describe:___________________________ ______________________________________________________________________________ In order for a family to be healthy or close, that family must… (Please fill in the blank): ______ ______________________________________________________________________________ In the section below identify if there is a family history of any of the following. If yes, please indicate the family member’s relationship to you in the space provided (father, grandmother, uncle, etc.) _Please Circle_________________List Family Member_____________ Alcohol/Substance Abuse ADD/ADHD Anxiety Disorder Adoption Bipolar Disorder Depression Domestic Violence Eating Disorder Learning Disabilities Obesity Obsessive Compulsive Behavior Panic Attacks Schizophrenia Sleep Disturbances Suicide Attempts Trauma History Please circle all of the issues which apply to you: Insomnia Memory Concentration Anger Stress Loneliness Drug use Anxiety Alcohol use Friends Family Fears Appetite Shyness Suicidal thoughts Phobias Mood swings Rapid speech Panic attacks Hallucinations Unexplained losses of time Depression Eating disorder Body image problems Self-control Health problems Sexual problems Legal matters Repetitive thoughts Repetitive behaviors Making decisions Homicidal thoughts Stomach problems Addiction Relationship Difficulties Self-esteem issues Cutting Grief over a loss Post abortion grief Other: _____________________________________________________________________