Detention under the Mental Health Act or Deprivation of Liberty

Clinical
Mental Health Act 1983 / Mental Capacity Act 2005:
Detention under the Mental Health Act or Deprivation of Liberty
Safeguards - Standard Operating Procedure
Document Control Summary
Status:
Replacement.
Replaces part of:
C-YEL-mh-ca-05 Use of the MCA
C-YEL-mh-ca-10 Assessment for Admission under the MHA
C-YEL-mh-ca-14 Deprivation of Liberty Safeguards
C-YEL-mh-ca-16 Informal Admission
Version:
Author/Owner/Title:
Approved by:
Ratified:
Related Trust Strategy and/or Strategic Aims
Implementation Date:
Review Date:
Key Words:
Associated Policy or
Standard Operating
Procedures v1.0 Date: 25.09.2015
Dawn Crowther, Mental Health Legislation Manager
Policy and Procedures Committee Date: 19/11/2015
Policy and Procedures Committee Date: 19/11/2015
Provide high quality recovery focused services.
Deliver regulatory, financial, performance and quality standards
November 2015
November 2018
Mental Health Act, MHA, Code of Practice, Section, Detention,
Formal, Informal, Hospital Managers, Mental Capacity Act, MCA,
Deprivation of Liberty Safeguards, DOLS, Admission
Policies
Conveyance
Mental Capacity Act 2005
Mental Health Act 1983
Standard Operating Procedures (SOPs)
Admission to hospital
Deprivation of Liberty Safeguards
Receipt of MHA documentation
Contents
Page 1 of 8
Process for Monitoring Compliance and Effectiveness ........................................ 8
Change Control
– Amendment History
Version Dates Amendments
1. Introduction
1.1 The Mental Health Act 1983 as amended by the Mental Health Act 2007 (MHA), together with the Mental Capacity Act 2005 (MCA), provides the legal framework by which individuals may be detained in order that they may receive care and treatment appropriate to address the needs of their mental disorder.
1.2 This procedure supersedes those detailed on the cover page to this document and must be read in conjunction with the statutory references at 6 below and the Trust Policies and Standing Operating Procedures on the Document Control Summary on the front pages of this document.
2. Purpose
2.1 The purpose of this document is to assist staff in identifying the appropriate statutory framework (MHA / MCA) by which patients may be assessed and treated and legally deprived of their liberty when appropriate.
3. Scope
3.1 The MHA and MCA policies should be referred to for the wider Trust roles in respect of the legislation.
3.2 This standard operating procedure relates to all staff responsible for and/or working with inpatients, or those patients being considered for inpatient care. It also informs staff from other agencies involved in the care and treatment of these patients.
All staff caring for patients should be familiar with the requirements of the MHA, MCA and related
Page 2 of 8
documents, and with proce dures detailed in the Trust’s SOPs. They must pay due regard to the MHA, MCA and DoLS Codes of Practice, apply the Codes ’ Guiding
Principles when carrying out their work, and ensure they keep up to date with MHA and
MCA practice commensurate with their role.
3.3 Specifically this document relates to the following groups who undertake direct key roles in the implementation and delivery of this procedure:
3.3.1 Team Leaders / Departmental Heads / Ward and Unit Managers are responsible for ensuring all staff are conversant with the MHA, MCA and DoLS
Codes of Practice, this procedure and related policies and SOPs. They must be aware of and ensure implementation of the processes and actions that are required to be taken in relation to patients in their service area. They must ensure that all employees in posts in the Trust clinical services are aware of their responsibilities in relation to the Acts and attend appropriate training commensurate with their role.
3.3.2 Medical Staff / Section 12(2) Approved Doctors / Approved Clinicians hold a key role in the processes and actions that are required to be taken in relation to detention and treatment of patients. They must be aware of this procedure and ensure implementation of the processes and actions that are required to be taken in relation to patients for whom they are responsible.
3.3.3 Registered healthcare professionals are accountable for their own practice and must be aware of legal and professional responsibilities relating to their competence, observe this procedure, legislation and guidance as detailed above, and work within the Code of Practice of their professional body.
3.3.4 Trust employees working in roles to provide healthcare in direct clinical contact with patients are responsible for carrying out procedures in line with the standards detailed in this and other related Trust’s SOPs and maintaining their individual competence in the practice of the Acts and attending training as required by their roles.
3.3.5 Approved Mental Health Professionals are accountable for their own practice and must be aware of legal and professional responsibilities relating to their competence, observe this procedures, legislation and guidance as detailed above, and work within the Code of Practice of their professional body.
3.3.6 The Mental Health Legislation Manager is responsible for the development, monitoring and review of this procedure and practice standards, disseminating new guidance as it arises and giving advice to all staff on MHA and MCA issues. This manager is also responsible for highlighting practice issues arising within the Trust, provision of appropriate administration support in relation to the Acts, education to support the policy standards, advising the
Page 3 of 8
Mental Health Legislation Committee that monitors the use of the Acts and reports to the Quality Governance Committee of any issues relating to the implementation of the MHA and MCA Policies and SOPs.
3.3.7
MHA Hospital Manager Panel Members
Power of discharge under section 23(4) of the Act is exercised by the Non-Executive
Directors of the Board and MHA Hospital Manager Panel Members as authorised by the Trust Board (see SOP for Hospital Managers). Panel Members must observe the requirements of the MHA and MCA Codes of Practice and the guidance contained in this and other related Trust MHA and MCA procedures whilst carrying out their duties.
4 Consideration of MHA/MCA/DOLS
4.1 Trust staff involved in the admission and care of patients within an inpatient setting must familiarise themselves with paragraphs 13.49 to 13.62 and 14.11 to 14.25 of the
MHA Code of Practice which provide guidance on consideration of the appropriate legal framework to be utilised to authorise care and treatment in any given circumstance.
4.2 In considering whether it is necessary for a patient to be detained under the MHA, decision makers must consider whether the person has capacity to consent to or refuse admission and treatment. This should be assessed in accordance with the
MCA, which makes it clear that a person must be assumed to have capacity unless it is established that they do not.
4.3 The MCA may be used to treat people for mental disorder when they cannot consent to the treatment because they lack capacity and where the treatment is in their best interests. Where the care and treatment of a person who lacks capacity amounts to a deprivation of their liberty, that deprivation must be authorised to be lawful, either under the Deprivation of Liberty Safeguards (DOLS), contained in the Mental
Capacity Act (MCA), or the Mental Health Act 1983 (MHA).
4.4 A patient who lacks capacity to consent to being accommodated in a hospital for care and/or treatment for mental disorder and who is likely to be deprived of their liberty should never be informally admitted to hospital (whether they are content to be admitted or not).
4.5 DoLS cannot be used if the patient is objecting to admission and / or treatment for their mental disorder – the MHA must be used if criteria for detention are fulfilled.
4.6 If there is any evidence of objection from the individual concerned, subtle objection or the patient is heavily sedated and is not in a position to voice objection or there is
Page 4 of 8
likely to be objection during the course of the care, then this would likely indicate that the patient will be ineligible for DoLS and the MHA will be the appropriate route.
4.7 Whether a patient is objecting has to be considered in the round, taking into account all the circumstances, so far as they are reasonably ascertainable. The decision to be made is whether the patient objects, the reasonableness of that objection is not the issue. In many cases the patient will be perfectly able to state their objection. In other cases the relevant person will need to consider the patient’s behaviour, wishes, feelings, views, beliefs and values, both present and past, so far as they can be ascertained. In deciding whether a patient objects to being admitted to hospital, or to some or all of the treatment they will receive there for mental disorder, decisionmakers should err on the side of caution and, where in doubt, take the position that a patient is objecting.
4.8 In cases of fluctuating capacity, where the individual may regain capacity and there is evidence that they would object to treatment, such a situation is likely to indicate use of the MHA to authorise a deprivation of liberty should be preferred over use of a
DoLS authorisation or Court of Protection order.
4.9 It is important to note that a person will be ineligible for a DoLS authorisation or a
Court of Protection order if they fall within Schedule 1A to the MCA. This includes:
• patients detained under sections 2, 3, 4, 35 – 38, 44, 45A, 47, 48 or 51 of the MHA
• patients on a community treatment order (CTO) under the MHA AND (i) proposed care and treatment in a hospital or care home would conflict with a condition of their CTO OR (ii) the relevant care and treatment consists in whole or in part of treatment for mental disorder in a hospital.
See paragraph 13.56 of the MHA Code of Practice for further information on exclusions.
4.10 The only situation where there is a choice between the regimes is when the patient lacks capacity, the care regime amounts to a deprivation of liberty, and they are not objecting.
4.11 For those individuals where both detention under the Act and a DoLS authorisation or a Court of Protection order are available, decision-makers should determine which regime is the more appropriate. The choice of legal regime should never be based on a general preference for one regime or the other, or because one regime is more familiar to the decision-maker than the other. In addition decision-makers should not proceed on the basis that one regime is generally less restrictive than the other. Both regimes are based on the need to impose as few restrictions on the liberty and autonomy of patients as possible. In the particular circumstances of an individual case, it may be apparent that one regime is likely to prove less restrictive. If so, this should be balanced against any potential benefits associated with the other regime.
Page 5 of 8
4.12 Both regimes provide appropriate procedural safeguards to ensure the rights of the person concerned are protected during their detention. Decision-makers should not therefore proceed on the basis that one regime generally provides greater safeguards than the other. However, the nature of the safeguards provided under the two regimes are different and decision-makers will wish to exercise their professional judgement in determining which safeguards are more likely to best protect the interests of the patient in the particular circumstances of each individual case.
4.13 In the relatively small number of cases where detention under the Act and a DoLS authorisation or Court of Protection order are available, The decision should always be made depending on the unique circumstances of each case.
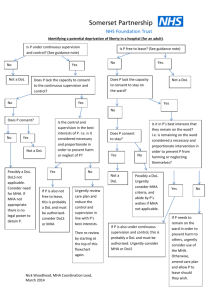
4.14 Figures 4a and 4b below provide further guidance on the utilisation of
MHA/MCA/DoLS.
Figure 4a
Availability of MHA /
DoLS Options Grid
Individual capacity to consent to being accommodated in a hospital for care and/or treatment
Individual treatment has lacks the the capacity to consent to being accommodated in a hospital for care and/or
Individual objects to the proposed accommodation in a hospital for care and/or treatment; or to any of the treatment they will receive there for mental disorder
Only the MHA is available
Only the available
MHA is
Individual does not object to the proposed accommodation in a hospital for care and/or treatment; or to any of the treatment they will receive there for mental disorder
The MHA is available.
Informal admission might also be appropriate.
Neither DoLS nor Court of Protection order available
The MHA is available.
DoLS authorisation is available, or potentially
Court of Protection Order
Page 6 of 8
Figure 4b
Deciding whether the
MHA / MCA / DoLS is available for use
Yes
Yes
Yes
No
No
No
No
Yes
Yes
No
Page 7 of 8
5
Recording
5.1 A record of whether a person is able to consent to admission must be made using
Form MCA2 within the MCA folder in the RiO electronic patient record where any person is admitted to hospital. The nurse in change of the ward is responsible for ensuring that this is completed within 24 hours of admission to hospital .
5.2 Where the implementation of DOLS procedures are indicated are necessary, please see the Trust SOP on Deprivation of Liberty Safeguards for further guidance.
5.3 The Trust Informal Admission SOP should be followed for patients admitted to hospital who are not subject to any form of detention.
5.4 Patients’ legal status must be kept under review by the Responsible Clinician (RC) /
Consultant in charge of the patients’ care. When changes in the regime to be used are indicated due to a change in the patients’ capacity to consent to the admission and / or treatment, a record of the reasons for the change must be recorded on form
MCA2.
6
Process for Monitoring Compliance and Effectiveness
Aspect of compliance or effectiveness being monitored
Monitoring method
Individual/ department responsible for the monitoring
Frequency of the monitoring activity
Group or committee/ forum which will receive the findings/ monitoring report
Committee/ individual responsible for ensuring that the actions are completed
Completion of
MCA2 for admission
Ward MHA audit check list
Ward
Managers
Monthly MHLM
7
References
Mental Health Act 1983 (amended 2007)
Mental Health Act 1983: Code of Practice (2015) Department of Health
Reference Guide to the Mental Health Act 1983 (2015)
Mental Capacity Act 2005 (amended 2007)
Mental Capacity Act 2005: Code of Practice (2007)
Mental Capacity Act: Deprivation of Liberty Safeguards Code of Practice (2008)
MHLC / QGC
Page 8 of 8