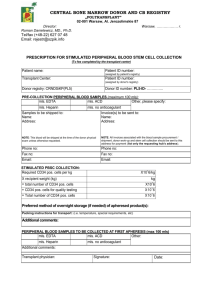
Prescription for Bone Marrow Collection
advertisement

ANTHONY NOLAN 2 Heathgate Place 75-87 Agincourt Road London NW3 2NU www.anthonynolan.org T:+ (44) 0303 303 0303 F: +(44) 0207 284 8226 Emergency: + (44) 07710 599161 E: donorprovision@anthonynolan.org Registered charity number 803716/SC038827 PRESCRIPTION FOR BONE MARROW COLLECTION (To be completed by the transplant centre) Recipient Initials: Recipient ID: (assigned by recipient’s TC/registry) Recipient ID: Recipient ID: (assigned by Anthony Nolan) (assigned by donor’s registry) Donor registry: Donor ID number: PRE-COLLECTION PERIPHERAL BLOOD SAMPLES (maximum 100 mls): mls. EDTA mls. ACD mls. Heparin mls. no anticoagulant Other, please specify: Samples to be shipped to: Name: Address: Product to be delivered to: Name: Address: NOTE: This blood will be drawn at the donor medical unless otherwise requested. Phone no: Phone no: Fax no: After hours number: Email: Fax no: BONE MARROW COLLECTION NUCLEATED CELLS PER KG (UNCORRECTED) X 10^8/kg x recipient weight (kg) kg = total nucleated cells for recipient (uncorrected) X 10^8 + nucleated cells for quality assurance X 10^8 = Total nucleated cells X 10^8 Ethics Approval Date (if appropriate) (day/month/year) Anticoagulant: Media for marrow transportation: Packing instructions for transport: (i.e. temperature, special requirements, etc) PERIPHERAL BLOOD SAMPLES TO BE COLLECTED AT TIME OF HARVEST(maximum 100 mls): mls. EDTA mls. ACD mls. Heparin mls. no anticoagulant Marrow: Additional comments: Transplant physician: Signature: Date: (day/month/year) DOC1103 Page 1 of 1 Version 004 (0515)