JACC113012-4898R: 2`end revision Supplementary Appendix J
advertisement

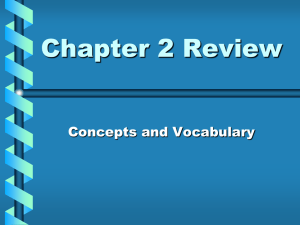
JACC113012-4898R: 2’end revision Supplementary Appendix J-shaped Association between QTc Interval Duration and the Risk of Atrial Fibrillation: Results from the Copenhagen ECG Study Supplementary Methods Danish Registers Using a unique personal identification number (the central personal registration [CPR] number) assigned to all persons with permanent residence in Denmark, it is possible to link data from multiple sources at an individual level.1 The Danish National Patient Register holds information on all hospital, ambulatory, and emergency room discharge diagnoses (International Classification of Diseases and Related Health Problems, revision 8 [ICD-8] from 1977-1993 and revision 10 [ICD10] from 1994 and onwards), including information on invasive procedures such as surgeries and percutaneous interventions (coded according to the Nordic Medical Statistics Committees Classification of Surgical Procedures since 1996).2 The Danish Register of Causes of Death holds information on any in-country death since 1970 (ICD-10 classified since 1994).3 The Register of Medicinal Products Statistics has information on an individual level for all dispensed prescription drugs sold in Denmark since 1995 (e.g., international anatomical therapeutic chemical classification system [ATC] code, strength, and quantity).4 Data on migrations is recorded in The Danish Civil Registration System.5 1 Medication Data The Danish Registry of Medicinal Product Statistics holds information on the dispensing date of the prescription, the strength of the drug, and the total quantity (e.g., number of tablets) dispensed, but not the prescribed dose of the drug.4 Under the assumption that individuals were receiving treatment when a drug was available (purchased), the period of time in which an individual was taking a particular drug (medication period) was estimated based on the World Health Organization defined daily dose (e.g., milligram/day) for the particular medication.4,6 Medication periods were considered overlapping if they were separated by less than 30 days. Study Population In the greater region of Copenhagen, Denmark, the vast majority of general practitioners have joined the Copenhagen General Practitioners’ Laboratory (CGPL) for the purpose of centralized large-scale production of various paraclinical procedures, such as biochemistry and electrocardiogram (ECG) recordings. At CGPL, standardized and high quality digital ECG recordings from a large proportion of the Copenhagen general population have been accumulated since 2001. In addition, a considerable amount of biochemical tests such as cholesterol profiles, glucose tests and thyroid profiles have been accumulated on this same population. The study population (The Copenhagen ECG Study) consists of all individuals who had an ECG recorded at CGPL at the behest of their general practitioner from 2001-2010. Study subjects were included at the day of first ECG recording. We excluded individuals for the following reasons (Figure 1): age less than 15 years, prior AF or atrial flutter (ICD-10 hospital, ambulatory, or emergency room discharge diagnosis I48.9), prior treatment with class I and III antiarrhythmic drugs or digoxin (ATC code C01B, C01AA, C07AA07), existing pacemaker or implantable cardioverter defibrillator (ICD; procedure code BFCA0, BFCA1, BFCA2, BFCA3, BFCA6, 2 BFCA7, BFCB0, BFCB2, BFCB3, BFCB5, BFCB6, BFCB7, ZZ4050, ZZ4051), and/or an inclusion ECG not consistent with analysis or a straightforward interpretation of the QT interval (see electrocardiography section). Comparison to the General Population To compare the ECG study population with the general population with respect to incidence rate of AF and mortality rate, we randomly sampled individuals from the entire Danish population (5.6 million), matched 1:2 based on gender and age at the time of inclusion. Poisson regression was used to compare rates per 1,000 person-years in the ECG study population with the sample from the general population. Electrocardiography All digitally recorded ECGs were stored in the MUSE® Cardiology Information System (GE Healthcare, Wauwatosa, WI, USA) and later processed using the latest version 21 of the Marquette 12SL algorithm.7,8 All ECGs were recorded at CGPL or at one of its satellite clinics according to a standardized protocol. According to this protocol, ECG technicians are instructed to inspect ECGs at the time of recording with the aim of detecting technical errors, missing leads, and inadequate quality, and to replace such recordings with a new ECG. In case of multiple ECGs on a single individual, only the first ECG recorded at CGPL (baseline ECG) was used. With the use of the 12SL algorithm statements and intervals we excluded ECGs with the following findings that were not consistent with a valid or straightforward measurement and interpretation of the QTc interval: AF, atrial flutter, bradyarrhythmias (heart rate < 40 beats per minute [b.p.m.]), tachyarrhythmias (heart rate > 110 b.p.m.), bundle branch blocks and ventricular rhythms (QRS 3 interval >120 milliseconds [ms]), delta waves, second and third degree AV-blocks, multiple premature ventricular complexes, multiple premature atrial complexes, junctional rhythms, pace spikes, and QTcFram intervals ±4 standard deviations from the mean (QTcFram <340ms or QTcFram >492ms). To obtain QT intervals, the Marquette 12SL algorithm constructs a representative median beat from all PQRST complexes in the 12 leads of the 10-second ECG tracing and annotates fiducial points on the superimposed medians.7,8 The QT interval measured by the 12SL algorithm essentially corresponds to the distance between the earliest detection of depolarization in any lead (QRS onset) and the latest detection of repolarization in any lead (T-offset). The algorithm excludes from the analysis any discrete U-waves that occur after the T-wave returns to baseline, whereas complex multiphasic T-waves and T-U complexes are included.7,8 QT intervals were corrected for heart rate using either Fridericia’s formula (QTcFrid = QT/RR1/3) or Bazett’s formula (QTcBaz = QT/RR1/2). Measurement of QTc intervals using the Marquette 12SL algorithm have previously been validated extensively.9,10,11 To validate our algorithm excluding ECGs with findings that were not consistent with a valid or straightforward interpretation of the QTc interval, we randomly sampled 200 ECGs for manual evaluation. The number of selected ECGs was based on a prior power calculation taking into consideration the expected proportion of ECGs with findings not consistent with a valid or straightforward interpretation of the QTc interval (α = 0.01, 95% power, estimated proportion = 5%, resulting in a minimum of N = 127 ECGs to be evaluated). From the proportion of randomly selected ECGs with findings not consistent with a valid or straightforward interpretation of the QTc interval, we estimated an upper exact 97.5% confidence limit for the presence of such ECGs in the entire ECG study population. 4 Clinical Covariates and Outcomes Hypertension was defined as present if an individual at some point prior to study inclusion was treated simultaneously with at least two of the following classes of antihypertensive drugs: beta adrenergic blockers (C07), alpha-blockers (C02A, C02B, C02C), calcium channel blockers (C07F, C08, C09BB, C09DB), inhibitors of the renin-angiotensin system (C09), non-loop diuretics (C02DA, C02L, C03A, C03B, C03D, C03E, C03X, C07C, C07D, C07G, C09BA, C09DA, C09XA52), and vasodilators (C02DB, C02DD, C02DG, C04, C05). This definition of hypertension has been used previously.12 Heart failure was defined as a combination of a heart failure diagnosis (I110, I42, I50, J819) in the Danish National Patient Registry and treatment with loop-diuretics (C03C), as done previously.12 Myocardial infarction was defined from hospital, ambulatory, and emergency room discharge diagnoses (ICD-8: 410, ICD-10: I21, I22).13 We categorized individuals as having valvular heart disease if they were assigned a diagnosis of aortic or mitral valve disease (I05, I06, I34, I35), or if they had aortic or mitral valve surgery (procedure code KFK and KFM).12 Diabetes at baseline was defined as a hospital, ambulatory, or emergency room discharge diagnoses of diabetes mellitus (E10, E11, E12, E13, E14), treatment with glucose-lowering drugs (A10), or an opportunistic blood sample at CGPL prior to study inclusion indicative of diabetes mellitus (hemoglobin A1c >6.5 mmol/L or plasma glucose ≥11.1 mmol/L). Similarly, hyperthyroidism was defined as a diagnosis of thyrotoxicosis (E05), treatment with antithyroid drugs (H03B), or a blood sample indicative of hyperthyroidism prior to inclusion (thyroid stimulating hormone <0.01 mmol/L in a subject not receiving thyroid therapy [H03AA]). Study subjects treated with QT interval prolonging drugs (yes/no, see Supplementary Table 1 for a complete list) on the day of the ECG recording were identified. A mean ratio of total to high density lipoprotein (total cholesterol/HDL) was calculated for the subset of study subjects from whom a cholesterol profile was taken at CGPL up to one year prior to study inclusion. A hospital, ambulatory, or emergency 5 room discharge diagnosis of AF or atrial flutter (ICD-10: I48.9) was the primary endpoint of interest. Supplementary Results Comparison to the General Population The incidence rate of AF was 6.7 (95% CI 6.5-6.8) per 1,000 person-years in the ECG study population compared with 5.3 (95% CI 5.3-5.4) in the general Danish population (matched 1:2 based on gender and age at the time of inclusion, P < 0.001). The all-cause mortality rate was 16.7 (95% confidence interval [CI] 16.5-16.9) per 1,000 person-years in the ECG study population and 16.0 (95% CI 15.8-16.1) in the sampled general population (P <0.001). Electrocardiographic Validations All sampled ECGs (200/200) were suitable for measurement of the QTc interval. Accordingly, no ECGs with bundle branch, pace spikes or arrhythmias except from single premature ventricular complexes or premature atrial complexes were detected. No technical errors, missing leads, or issues related to inadequate quality to an extent that could hinder a precise QTc interval estimation were observed. All ECGs displayed sinus rhythm, except three that displayed an ectopic atrial rhythm. Using these data and a one-sided 97.5% confidence limit resulted in an upper confidence level of 1.8% of the ECGs that were not consistent with valid measurement of the QTc interval. The 200 sampled ECGs had a median QTcFram interval of 417ms (IQR 404-433ms) and a range of 350482ms. 6 Supplementary References 1. Frank L. When an entire country is a cohort. Science. 2000;287(5462):2398–2399. 2. Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39(7 Suppl):30–33. 3. Helweg-Larsen K. The Danish Register of Causes of Death. Scand J Public Health. 2011;39(7 Suppl):26–29. 4. Kildemoes HW, Sørensen HT, Hallas J. The Danish National Prescription Registry. Scand J Public Health. 2011;39(7 Suppl):38–41. 5. Pedersen CB. The Danish Civil Registration System. Scand J Public Health. 2011;39(7 Suppl):22–25. 6. Anon. WHOCC - ATC/DDD Index. Available at: http://www.whocc.no/atc_ddd_index/. Accessed March 2, 2012. 7. GE Healthcare. MarquetteTM 12SLTM ECG Analysis Program. Statement of Validation and Accuracy. 416791-003 Revision C. Available at: http://gehealthcare.com. Accessed April 2, 2012. 8. GE Healthcare. MarquetteTM 12SLTM ECG Analysis Program. Physician’s Guide. 2036070-006 Revision A. Available at: http://gehealthcare.com. Accessed April 2, 2012. 9. Rautaharju PM, Prineas RJ, Kadish A, et al. Normal standards for QT and QT subintervals derived from a large ethnically diverse population of women aged 50 to 79 years (the Women’s Health Initiative [WHI]). Am. J. Cardiol. 2006;97(5):730–737. 10. Hnatkova K, Gang Y, Batchvarov VN, Malik M. Precision of QT interval measurement by advanced electrocardiographic equipment. Pacing Clin Electrophysiol. 2006;29(11):1277–1284. 11. Fosser C, Duczynski G, Agin M, Wicker P, Darpo B. Comparison of manual and automated measurements of the QT interval in healthy volunteers: an analysis of five thorough QT studies. Clin. Pharmacol. Ther. 2009;86(5):503–506. 12. Olesen JB, Lip GYH, Hansen ML, et al. Validation of risk stratification schemes for predicting stroke and thromboembolism in patients with atrial fibrillation: nationwide cohort study. BMJ. 2011;342:d124. 13. Madsen M, Davidsen M, Rasmussen S, Abildstrom SZ, Osler M. The validity of the diagnosis of acute myocardial infarction in routine statistics: a comparison of mortality and hospital discharge data with the Danish MONICA registry. J Clin Epidemiol. 2003;56(2):124–130. 7 Supplementary Table 1. QTc Interval Prolonging Drugs by ATC code Drug category Drugs (ATC code) Alimentary tract and metabolism Domperidone (A03FA03), Ondansetron (A04AA01), Granisetron (A04AA02) Cardiovascular system* Indapamide (C03BA11), Isradipine (C08CA03), Nicardipine (C08CA04), Moexipril (C09AA13) Urogenital system Solifenacin (G04BD08), Vardenafil (G04BE09), Alfuzosin (G04CA01, G04CA51) Antibiotics Trimethoprim-Sulfa (J01EA01), Erythromycin (J01FA01), Roxithromycin (J01FA06), Procainamide (J01FA09), Azithromycin (J01FA10), Ofloxacin (J01MA01), Ciprofloxacin (J01MA02), Moxifloxacin (J01MA14), Ketoconazole (J02AB02), Fluconazole (J02AC01), Itraconazole (J02AC02), Voriconazole (J02AC03) Antineoplastic and immunomodulatory agents Tamoxifen (L02BA01), Tacrolimus (L04AD02) Muscle and skeletal system Tizanidine (M03BX02) The nerve system Amantadine (N04BB01), Thioridazine (N05AC02), Haloperidol (N05AD01), Sertindole (N05AE03), Ziprasidone (N05AE04), Pimozide (N05AG02), Clozapine (N05AH02), Quetiapine (N05AH04), Lithium (N05AN01), Risperidone (N05AX08), Paliperidone (N05AX13), Chlorpromazine (N05AA01), Fluoxetine (N06AB03), Citalopram (N06AB04), Paroxetine (N06AB05), Sertraline (N06AB06), Escitalopram (N06AB10), Venlafaxine (N06AX16), Galantamine (N06DA04), Imipramine (N06AA02, N06AA02), Clomipramine (N06AA04), Trimipramine (N06AA06), Amitriptyline (N06AA09), Nortriptyline (N06AA10), Protriptyline (N06AA11), Doxepin (N06AA12), Methadone (N07BC02) Antiparasitic drugs, insecticides, and repellents Chloroquine (P01BA01), Pentamidine (P01CX01) Respiratory system Astemizole (R06AX11), Terfenadine (R06AX12), Diphenhydramine (R06AA02) The table lists all drugs associated with QT interval prolongation as listed on www.qtdrugs.org (accessed 7th of April 2011) and available in Denmark prior to 2011. *Individuals treated with QT interval prolonging antiarrhythmic drugs prior to or at the day of inclusion were excluded at baseline and for this reason these drugs are not listed. ATC; international anatomical therapeutic chemical classification system. 8 Supplementary Figure Legends Supplemental Figure 1 Multivariable-adjusted restricted cubic spline analysis showing the hazard ratio of AF as a function of QTcFram interval. Model 1 is identical to the AF model for the combined population shown in Figure 3A. Model 2 represents the proportion of the population where a baseline cholesterol profile was available. In this subgroup analysis, 157,919 individuals (56% of the study population) were included at baseline and 5,366 individuals developed AF. The model was adjusted for gender, hypertension, heart failure, myocardial infraction, valvular heart disease, diabetes, hyperthyroidism, PR interval (low <140 ms, medium 140-180 ms, and high >180 ms), left ventricular hypertrophy according to the Sokolow-Lyon ECG criteria, and treatment with QTc-prolonging drugs at the day of inclusion (yes/no). Model 3 is identical to model 2, but is additionally adjusted for the ratio of total to HDL cholesterol. The horizontal dotted line represents a hazard ratio of 1. QT intervals were heart rate corrected using the Framingham formula (QTcFram). In Model 4; which is based on the total study population, status regarding hypertension, heart failure, myocardial infraction, valvular heart disease, diabetes, and hyperthyroidism were updated over time. 9 Supplemental Figure 1 10