Carbon Monoxide Poisoning
advertisement

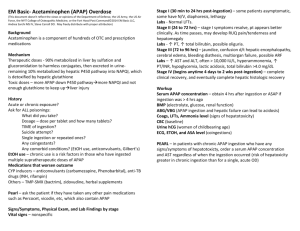
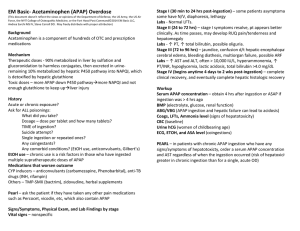
Manini 8/4/05 Acetaminophen Poisoning Intro/Scope: Other common names: paracetamol, N-acetyl-para-aminophenol (APAP) Most commonly reported potentially toxic agent Greatest absolute number of toxic fatalities in US Extremely common co-ingestant APAP is leading cause of admission to liver transplant units in US (2003 study). What happens in Overdose? Sulfation and glucuronidation pathways become saturated APAP shunted to P450 pathway, resulting in NAPQI, a highly reactive and toxic intermediate. Increase in NAPQI depletes glutathione stores NAPQI binds nonspecifically to intracellular proteins, resulting in general cell dysfunction. Signs and Symptoms: Stage I (30 min-24 hr): pallor, diaphoresis, n/v, abd pain, anorexia, malaise. Stage II (24-48 hr): Resolution of stage I sx/signs, RUQ pain, liver/renal dysfunction Stage III (72-96 hr): jaundice, peak LFTs, hepatic/renal failure, death. Stage IV (4 d – 2 wk): fulminant hepatic failure, coma, death OR resolution of hepatotoxicity Evaluation of Toxicity: 150 mg/kg is potentially toxic dose Serum APAP level at 4 hours post-ingestion Send serum APAP in ALL CASES of toxic ingestion: 1/500 pts without a history of APAP ingestion will have a toxic level. APAP treatment nomogram – cannot be applied to levels obtained before 4 hours. (see Figure below) Treatment: Consider orogastric lavage for co-ingestants – typically only for intubated pts Activated Charcoal (AC) – 1gm/kg for patients without contraindications (To wit: decreased gut motility, perforated viscous, endoscopy planned, or not protecting airway). If multi-dose AC is indicated for co-ingestants, stagger doses with PO NAC by 2 hrs to avoid potential interference, although there is evidence this is not clinically significant. N-acetylcysteine (NAC) – administer this early (< 8 hrs): early NAC was equally efficacious regardless of how high the serum APAP level was. (Smilkstein, 1988) o PO Dosing (Mucomyst): 72 hr protocol Load: 140 mg/kg Maintenance: 70 mg/kg q 4 hr x 17 doses o IV Dosing (Acetadote): 20 hr protocol Load: 150 mg/kg in 200 cc D5W over 15 min to 1 hr. Adverse effects are probably rate related, so there is still disagreement on this. Label says 15 min is safe, but some experts think 1 hr is safer. Next 4 hr: 50 mg/kg in 500 cc D5W Next 16 hr: 100 mg/kg in 1L D5W o IV vs PO NAC: IV NAC is used in all studies that demonstrate a benefit in hepatic failure. PO ass’d with emesis, which may cause aspiration. Co-ingestants may alter gut motility, favoring IV. IV protocol is shorter (20 hr vs 72 hr), saving 52 hr of hospital LOS. PO has fewer side effects than IV (rash, angioedema, anaphylactoid reactions). Manini 8/4/05 Fulminant Hepatic Failure: IV NAC dramatically improves survival if started before 8 hrs. Continue NAC until recovery from encephalopathy or patient expires. King’s College Criteria (O’Grady, 1991): o pH < 7.3 AND any of the following: PT >100, Creat > 3.0, Encephalopathy o Patients meeting criteria have 15% survival rate if not transplanted. Other prognostic markers: lactate >3 (Bernal, 2002), low phosphate (Schmidt, 2002) Supportive Care: treat bleeding, cerebral edema, infections, multi-organ system failure APAP Nomogram Manini 8/4/05 Study Questions 1. The toxic intermediate N-acetyl-p-benzoquinoneimine is formed via which pathway? . . . . . a. Sulfation . . . . . b. Glucuronidation . . . . . c. Cytochrome P-450 . . . . . d. Glutathionation 2. True/False: An adolescent presents with an acute ingestion of acetaminophen 5 hours prior. She is lethargic and is not responding appropriately. This clinical presentation is due to the acetaminophen toxicity. 3. N-acetylcysteine is most effective if given within how many hours of the acetaminophen ingestion? 4. Which is the first clinical stage that liver function tests may be abnormal? . . . . . a. Stage I . . . . . b. Stage II . . . . . c. Stage III . . . . . d. Stage IV 5. A patient arrives to the emergency department 7 hours after intentionally ingesting an unknown amount of acetaminophen. What should be done? . . . . . a. Directly admit the patient to the floor and await a psychiatric consult. . . . . . b. Draw a stat acetaminophen level and await the result before further treatment. . . . . . c. Give the patient syrup of ipecac if she has not vomited and then administer activated charcoal. . . . . . d. Draw a stat acetaminophen level and administer NAC. Suggested Reading 1. Keays R, et al. Intravenous actetylcysteine in paracetamol induced fulminant hepatic failure: a prospective controlled trial. Br Med J. 303:1026-1029. 2. O’Grady JG et al. Liver transplantation after paracetamol overdose. Br Med J 303:217-9, 1984. 3. Smilkstein MJ et al. Efficacy of oral N-acetylcysteine in the treatment of acetaminophen overdose. Analysis of the National Multicenter Study. NEJM 319: 1557-62, 1988. 4. Bizovi KE, Parker SJ, Smilkstein MJ. Chapter 142 - Acetaminophen. In: Marx JA (ed). Rosen's Emergency Medicine Concepts and Clinical Practice, fifth edition. 2002, St. Louis: Mosby Year Book, pp. 2069-2075. 5. Smilkstein MJ. Chapter 31 Acetaminophen. In Goldfrank LR, Flomenbaum NE, Lewin NA, Weisman RS, Howland MA, Hoffman RS (eds). Goldfrank's Toxicologic Emergencies, sixth edition. 1998, Stamford: Appleton & Lange; pp. 541-564. Manini 8/4/05 Answers to questions 1. c 2. False. Acute ingestion of acetaminophen does not cause altered mental status. 3. 8 hours 4. b 5. d