Top of Form All Sources eMedicine Medscape Drug Reference MEDLINE
advertisement

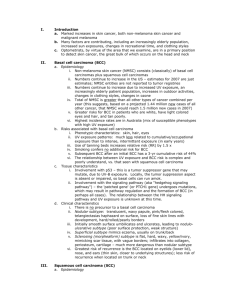
HOME SPECIALTIES REFERENCE CENTERS Search: eM Search You are in: eMedicine Specialties > Otolaryngology and Facial Plastic Surgery > Pathology Quick Find Author Information Introduction Clinical Differentials Workup Treatment Last Updated: December 11, 2006 Follow-up Synonyms and related keywords: basal cell carcinoma of the skin, BCC, basal cell Miscellaneous epithelioma, rodent ulcer, squamous cell carcinoma, SCC, nodular basal cell Pictures carcinoma, noduloulcerative basal cell carcinoma, morpheaform basal cell carcinoma, Bibliography sclerosing basal cell carcinoma, superficial basal cell carcinoma, basosquamous carcinoma, basisquamous carcinoma, basal squamous cell carcinoma, skin BCC Skin Cancer: Basal Cell Carcinoma AUTHOR INFORMATION Email to a Colleague Section 1 of 10 Author Information Introduction Clinical Differentials Workup Treatment Follow-up Miscellaneous Pictures Bibliography Click for related images. Related Articles [Squamous Cell Author: M Abraham Kuriakose, MD, DDS, FRCS, Chairman, Head Carcinoma of the and Neck Institute, Amrita Institute of Medical Sciences Skin] M Abraham Kuriakose, MD, DDS, FRCS, is a member of the following medical societies: American Head and Neck Society, British Association of Oral and Maxillofacial Surgeons, and Royal College of Surgeons of England Patient Education Editor(s): Jaime R Garza, MD, DDS, FACS, Consulting Staff, Private Cancer and Practice; Francisco Talavera, PharmD, PhD, Senior Pharmacy Editor, Tumors Center eMedicine; Karen Hall Calhoun, MD, Chair, Professor, Department of Otolaryngology-Head and Neck Surgery, University of Missouri; Skin Cancer Overview Christopher L Slack, MD, Otolaryngology-Facial Plastic Surgery, Private Practice, Associated Coastal ENT; Medical Director, Treasure Skin Cancer Coast Sleep Disorders; and Arlen D Meyers, MD, MBA, Professor, Causes Department of Otolaryngology-Head and Neck Surgery, University of Colorado School of Medicine Skin Cancer Symptoms Disclosure Skin Cancer Treatment Skin Biopsy Introduction Skin Biopsy Preparation INTRODUCTION Section 2 of 10 Author Information Introduction Clinical Differentials Workup Treatment Follow-up Miscellaneous Pictures Bibliography Background: Basal cell carcinoma (BCC) constitutes approximately 80% of all nonmelanoma skin cancers. The tumors most often appear in individuals aged 40-60 years. BCC's predilection for the head and neck is notable and is related to its primary etiology—solar exposure. Approximately 75-86% of primary BCCs are found on the head or neck. The most common location on the head is the nose, specifically the nasal tip and alae. Australia has the highest incidence of basal cell carcinoma in the world. Sun exposure is the primary etiologic agent for the development of BCC. Risk is related to skin type and the degree of exposure to sunlight, particularly UV-B radiation. The tumors are more frequent in individuals with fair complexions. Fitzpatrick skin-type scale, which ranges from very fair (skin type I) to very dark (skin type VI), categorizes cutaneous sensitivity to UV radiation. It is based on the individual's tendency to burn and tan and is a good predictor of relative risk among whites. The prevalence of BCC increases in areas of higher altitude and in areas of lower latitude. The incidence of BCC is rising, partly because of atmospheric changes and the increased popularity of sunbathing. Pathophysiology: BCC primarily affects sun-exposed skin, particularly the upper two thirds of the face. Frequency: In the US: For statistical purposes, BCC and squamous cell carcinomas (SCCs) are grouped as nonmelanoma skin cancer. Incidence of non-melanoma skin cancer varies depending on geographic location. These cancers cause about 300 cases per 100,000 population in Texas and Arizona. The incidence is about half that figure in New York and Maine. Internationally: Australia has the highest incidence of BCC, ranging from 650-1560 cases per 100,000 population. Mortality/Morbidity: The estimated annual death rate from this tumor is 0.44 per 100,000 persons. Most of these deaths are due to SCC. BCC rarely causes death. Morbidity is associated with uncontrolled advanced disease. Race: Whites of Celtic ancestry have the highest risk for BCC. Incidence is low in blacks, Asians, and Hispanics. Sex: BCC has a male predilection, with a 2:1 male-to-female ratio. Age: Incidence peaks in persons aged 55-75 years. CLINICAL Section 3 of 10 Author Information Introduction Clinical Differentials Workup Treatment Follow-up Miscellaneous Pictures Bibliography History: BCC appears as insidious, painless, nonhealing ulcers or nodules on the sun-exposed parts of the body. BCC has a particular predilection for the upper two thirds of the face and is common among white men who are elderly. Because of changing sun-exposing lifestyle patterns among the sexes, the male sex predilection is gradually decreasing. During the clinical evaluation, the patient's social and occupational history of sun exposure, family history of skin cancer, and geographic area of origin are determined to estimate the likelihood that a second primary tumor will develop. Obtain a past history of treatment of the index tumor or other skin tumors. In patients with recurrent tumors, deeper invasion should be expected. Recurrence following radiation therapy is often biologically more aggressive. Physical: Physical examination should attempt to elicit the subtype of BCC, extent of the tumor, and involvement of important cosmetic and functional structures. Palpation should be used to attempt to estimate the depth of invasion and fixation to the underlying structures. In patients with recurrent or deeply infiltrative tumors, involvement of the facial nerve or branches of the trigeminal nerve should be tested. Facial nerve function can be monitored by comparing facial symmetry during voluntary facial movements with that at rest. Sensory nerve function can be tested and compared to the nonaffected side by means of light touch and pinprick. Orbital invasion can cause diplopia, proptosis, and ophthalmoplegia. Any limitation in ocular movements and/or diplopia should be tested. BCC seldom causes regional or distant metastasis, with the exception of the metatypical basosquamous type. To evaluate for lymph node metastasis, particular attention should be taken to examine the parotid posterior auricular, suboccipital, and upper cervical groups of lymph nodes. Four different clinicopathologic types of BCC exist, each with distinct biologic behavior. Undifferentiated BCC Nodular or noduloulcerative BCC o o More than 60% of BCCs belong to this subtype. These lesions appear as well-circumscribed, domeshaped, pearly nodules with or without ulceration. Superficial BCC o This BCC subtype appears as a red scaly patch that resembles the chronic dermatitis predominantly seen in the extremities. o These tumors spread superficially and can involve a large surface area. o Although satellite islands appear multifocal on standard histopathologic examination, 3-dimensional reconstruction shows that they are interconnected. Morpheaform or sclerosing BCC o This form accounts for 10% of lesions. o Lesions appear as flat or slightly depressed, fibrotic, and firm. o The tumor has a deeply infiltrative character, which may extend beyond the clinically obvious tumor. This feature increases the recurrence potential of morpheaform or sclerosing BCC. Micronodular BCC o This type manifests as a plaquelike indurated lesion with poorly demarcated contours. o Other BCCs o o o They have increase incidence of recurrence and an aggressive behavior. Aggressive-growth BCC Infiltrative-growth BCC Metatypical BCC Differentiated BCCs o Keratotic BCC o Infundibulocystic BCC o Follicular BCC o Pleomorphic BCC Causes: Incidence of BCC correlates with the amount of accumulated sun exposure. Epidemiologic and molecular studies have confirmed that the UV radiation (UVR) spectrum of sunlight, in synergy with genetic susceptibility, is responsible for BCCs. UV radiation o The UVR spectrum of sunlight is divided into 3 parts: long wave UV-A (320-400 nm), intermediate wave UV-B (290320 nm), and shortwave UV-C (200-290 nm). UV-B and UV-C can modify unsaturated chemical bonds of nucleic acids, which may lead to mutations. UV-C does not penetrate the atmospheric ozone layer; therefore, UV-B is the primary agent responsible for most skin cancers. The UV-A spectrum is absorbed by melanin and, through free-radical transfer, affects cellular deoxyribonucleic acid (DNA). o Mutations caused by UVR typically include cytosine (C) to thymine (T) or CC to TT translocation. This process can cause activation of oncogenes or inactivation of tumor suppressor genes, leading to tumor initiation and progression. Host factors o In addition to environmental factors, host factors play a critical role in the pathogenesis of BCC. Host factors include racial predilections, genetic syndromes, predisposing syndromes, and immunologic factors. o Racial and ethnic factors White race with Celtic ancestry (eg, Irish, Scottish, Welsh) has the highest predilection for BCC. Predilection is primarily related to the pigmentary characteristics of the skin and sun sensitivity. Ability to tan is the most important protective factor. Light eye color; red, blonde, or light-brown hair color; and freckling are strong predictors of BCC. o Genetic syndromes Xeroderma pigmentosa is a rare autosomal recessive disorder characterized by hypersensitivity to UVR. It causes defects in DNA repair and synthesis, resulting in cutaneous cancers (eg, BCC, SCC, melanoma). Nevoid basal cell syndrome is an autosomal dominant disorder associated with multiple BCCs, odontogenic keratocysts, calcification of falx cerebri, and rib abnormalities. Epidermodysplastic verruciformis is an autosomal recessive disorder characterized by the development of BCC and SCC from warts. Molecular alterations o Inappropriate activation of the hedgehog (HH) signaling pathway is found in both sporadic and familial cases of BCC. This results in loss-of-function mutations in tumorsuppressor protein patched homologue 1 (PTCH1) and gain-of-function mutations in SHH, SMO, and GLI. o Mutations in TP53 are found in about 50% of sporadic cases. Most show signature mutations that indicate exposure to UV-B radiation. DIFFERENTIALS Section 4 of 10 Author Information Introduction Clinical Differentials Workup Treatment Follow-up Miscellaneous Pictures Bibliography [Squamous Cell Carcinoma of the Skin] Other Problems to be Considered: Eczema Psoriasis Actinic keratitis WORKUP Section 5 of 10 Author Information Introduction Clinical Differentials Workup Treatment Follow-up Miscellaneous Pictures Bibliography Imaging Studies: Perform diagnostic imaging studies for advanced tumors when there is question of invasion or involvement of underlying soft tissue or bone. CT scanning with bone windows is the imaging study of choice. As incidence of nodal metastasis is very low, evaluation of the neck is not essential. For early BCC, clinical examination suffices to determine extent of lesion. Other Tests: Photo documentation Procedures: Obtain a biopsy of the tumor to confirm the diagnosis and determine the histologic subtypes. Complete an incision or punch biopsy prior to definitive treatment. o Obtain the biopsy from the margins of the lesion to include both tumor and normal tissue. o A shave biopsy may be difficult to interpret because of tangential sectioning and should be avoided. Histologic Findings: The basaloid appearance of the epithelial islands is the pathognomonic feature of BCC. The cells mimic germinative epithelium and have an increased nuclear cytoplasmic ratio. These cells show peripheral palisading, in which they are arranged perpendicular to the basement membrane. The tumor has a characteristic invasive pattern with the formation of large islands, cords, and teardrops. Cells within the center of the epithelial islands have nondiscrete cytoplasmic borders and mimic syncytium. The cells do not have prominent nucleoli and lack intercellular bridges. The stomas show varying amounts of collagen deposition with abundant mucin. Staging: Primary tumor TX: Primary tumor cannot be assessed. o T0 - No evidence of primary tumor o T1 - Tumor 2 cm or less in greatest dimension o T2 - Tumor more than 2 cm but not more than 5 cm in greatest dimension o T3 - Tumor more than 5 cm in greatest dimension o T4 - Tumor invading deep extradermal structures Regional lymph node NX: Regional lymph node cannot be assessed. o N0 - No regional lymph node metastasis o N1 - Regional lymph node metastasis Distant metastasis MX: Presence of distant metastasis cannot be assessed. o M0 - No distant metastasis o M1 - Distant metastasis TREATMENT Section 6 of 10 Author Information Introduction Clinical Differentials Workup Treatment Follow-up Miscellaneous Pictures Bibliography Medical Care: The treatment of BCC is surgical. Chemotherapy does not play a role in the management of BCC. In patients with unresectable tumors, radiotherapy may be attempted as palliative treatment. Radiotherapy may be considered as an adjuvant to surgery in patients with advanced tumors or as a definitive treatment in selected patients with early tumors. Surgical Care: Curettage, cryotherapy, and laser ablation may be used to treat small superficial BCC. Surgical excision with a margin of normal tissue is generally recommended for all other lesions. This practice allows histologic examination of the specimen for confirmation of the adequacy of excision. Surgery also provides a high cure rate. Excise early tumors with a margin of normal tissue; the defect can be closed primarily or with skin grafts or local flaps. Advanced-stage tumors require a multidisciplinary approach, involving head and neck surgical oncologists, Mohs micrographic surgeons, pathologists, reconstructive plastic surgeons, prosthodontists, and anaplastologists. Neurosurgeons, ophthalmic surgeons, and radiotherapists may be included in selected patients. The principal aim of surgical treatment is to obtain complete excision of tumor with uninvolved margins. Cosmetic and functional concerns are secondary. The extent of surgical margin required depends on the histologic types. Although tumor clearance can be achieved with a narrow margin in noduloulcerative BCC, morpheaform BCC requires a wider margin. Expect deeper and/or wider infiltration in tumors arising in the midface, patients with a previous history of radiation, and patients with recurrent tumors. Smaller tumors can be excised in the clinic under local anesthesia with or without sedation. Larger lesions or lesions involving selected anatomic subsites (eg, eyelids) are best managed in the operating room. Two distinct surgical approaches are practiced in BCC excisions: en bloc excision and Mohs micrographic surgery. In the first option, perform en bloc surgical resection with the aim to remove tumor with a clear margin. After clearly orienting the specimen, check margins by using frozen section. Histologic studies have confirmed that the subclinical extension of disease varies from 1-6 mm. Tumors larger than 2 cm have wider subclinical invasion than smaller lesions; therefore, a tumor smaller than 2 cm requires a margin of only 4 mm to achieve adequate clearance. Larger morpheaform BCC requires a resection margin of 12 cm. The incidence of recurrence following surgical excision is 30% for patients with positive margin, 12% with close margin, and less than 5% for complete excision. In Mohs micrographic surgery, excise the tumor with close margins and process specimens by using frozen section. This technique identifies the precise anatomic location of the residual tumors, which then can be re-excised. By serial frozen section examination and re-excision, this procedure allows complete excision of tumor and limited removal of normal structures, thereby preserving function and cosmoses without compromising the cure rate. Mohs micrographic surgery is a labor-intensive procedure. Current indications of Mohs micrographic surgery are recurrent tumors, tumors larger than 2-cm diameter, morpheaform BCC, and tumors located at the high-risk periorbital and nasal region. Depending on complexity of the procedure, the principle of reconstructive ladder may be followed in reconstructing BCC surgical defects. This principle includes allowing healing by means of secondary intention, primary closure, skin graft, local flap, free flap, or prosthesis use. The reconstructive procedure can be performed concurrent with surgery or as a secondary procedure after obtaining final pathologic result. Consultations: Although early BCC can be treated adequately by means of local excision, advanced and recurrent tumors are best managed by a multidisciplinary approach involving head and neck surgical oncologists, Mohs micrographic surgeons, reconstructive plastic surgeons, pathologists, prosthetists, and radiation oncologists. During the initial consultation, counsel the patient regarding the extent of resection, type of reconstructive procedure, and attendant morbidity. Attach great importance to adequately preparing the patient regarding the cosmetic and functional result of treatment. During posttreatment follow-up, counsel the patient regarding sunlight exposure and the risk of second primary skin tumors. Diet: No dietary restrictions are indicated. Activity: No restrictions in physical activities are indicated. To prevent second primary skin tumors, counsel the patient to avoid lifestyles that risk excessive sunlight exposure. FOLLOW-UP Section 7 of 10 Author Information Introduction Clinical Differentials Workup Treatment Follow-up Miscellaneous Pictures Bibliography Further Inpatient Care: The reconstruction of the surgical defect may be performed concurrent with the primary resection or following the final pathology result as a second procedure. Further Outpatient Care: Patients with BCC require lifelong follow-up care. In the initial period, perform close examination of the primary tumor site to detect recurrence at an early stage. During follow-up, examine the sun-exposed area of the skin to identify second primary tumors. A general follow-up schedule calls for a 2-3 month intervals for 2 years, with annual follow-up thereafter. Deterrence/Prevention: Prevention of BCC centers on measures to decrease UVR exposure. The peak period of UVR occurs from 10 AM to 4 PM. Lifestyle modification, protective clothing, and use of sunscreen preparations with a protective factor of 15 or more should be considered. Initiation of preventive measures from childhood decreases the incidence of BCC. Patients with a high risk for BCC (eg, whites with Celtic ancestry), a previous history of BCC, or a lifestyle involving excessive sun exposure should be screened for BCC. Complications: Early postoperative complications o Bleeding o Infection o Loss of skin graft Late postoperative complications o Facial scar o Ectropion o Epiphora o Tumor recurrence Prognosis: Incidence of recurrence following surgical excision is 30% in patients with a positive margin, 12% in patients with a close margin, and less than 5% in patients with a complete excision. With adequate treatment, a cure rate of more than 95% can be expected. Recurrent tumors following radiotherapy have a low tumor control rate. Patient Education: Counsel patients regarding the need for preventive measures to decrease UVR exposure. The peak period of UVR occurs from 10 am to 4 pm. Advise patients to wear of protective clothing and the use of sunscreen preparations with a protective factor of 15 or more. For excellent patient education resources, visit eMedicine's Cancer and Tumors Center. Also, see eMedicine's patient education articles Skin Cancer and Skin Biopsy. MISCELLANEOUS Section 8 of 10 Author Information Introduction Clinical Differentials Workup Treatment Follow-up Miscellaneous Pictures Bibliography Medical/Legal Pitfalls: Early BCC is an indolent lesion, which may be confused with other benign dermatologic conditions, thus delaying diagnosis. Rule out BCC in elderly patients who have any persistent nodular or scaly lesions in the upper two thirds of the face. Adequate excision of BCC results in a much wider defect than the clinical lesion. Adequately prepare patients for the functional and aesthetic results of surgery. During postoperative surveillance, take care to detect early recurrence and new BCCs. Diagnosis of early recurrence may be difficult because of surgical scarring, fibrosis, and the presence of skin graft. Delay in diagnosis of tumor recurrence can affect the success of salvage treatment and its functional and aesthetic results. PICTURES Section 9 of 10 Author Information Introduction Clinical Differentials Workup Treatment Follow-up Miscellaneous Pictures Bibliography Caption: Picture 1. Basal cell carcinoma of the skin. A 68-year-old patient presenting with an advanced basal cell carcinoma (BCC) of the right periorbital region (frontal view). View Full Size Image Picture Type: Photo Caption: Picture 2. Basal cell carcinoma of the skin. Lateral view of face showing extent of tumor. View Full Size Image Picture Type: Photo Caption: Picture 3. Basal cell carcinoma of the skin. Intraoperative view outlining the extent of resection (lateral view). The surgical resection consisted of zygomatic bone and the lateral orbit. The eye was spared. View Full Size Image Picture Type: Photo Caption: Picture 4. Basal cell carcinoma of the skin. Intraoperative view showing the extent of resection (inferior view). View Full Size Image Picture Type: Photo Caption: Picture 5. Basal cell carcinoma of the skin. The surgical defect was reconstructed using a sensate osteocutaneous radial forearm free flap. The osteotomized radial form was used to reconstruct the zygomatic bone and the lateral orbital rim. To provide sensation to the flap, the antebrachial cutaneous nerve was anastomosed to branches of the trigeminal nerve. View Full Size Image Picture Type: Photo Caption: Picture 6. Basal cell carcinoma of the skin. Nodular basal cell carcinoma. Nodular aggregates of basalioma cells are present in the dermis and exhibit peripheral palisading (PP) and retraction artifact (RA). Melanin is also present within the tumor and in the surrounding stroma, as seen in pigmented basal cell carcinoma. Image courtesy Michael L. Ramsey, MD. View Full Size Image Picture Type: Photo Caption: Picture 7. Basal cell carcinoma of the skin. Scale, erythema, and a threadlike raised border are present in this superficial basal cell carcinoma on the trunk. Image courtesy Michael L. Ramsey, MD. View Full Size Image Picture Type: Photo Caption: Picture 8. Basal cell carcinoma of the skin. Larger superficial basal cell carcinoma. Image courtesy Michael L. Ramsey, MD. View Full Size Image Picture Type: Photo Caption: Picture 9. Basal cell carcinoma of the skin. Histology of superficial basal cell carcinoma. Nests of basaloid cells are seen budding from the undersurface of the epidermis. Image courtesy Michael L. Ramsey, MD. View Full Size Image Picture Type: Photo Caption: Picture 10. Basal cell carcinoma of the skin. Pigmented basal cell carcinoma has features of nodular basal cell carcinoma with the addition of darker pigmentation from melanin deposition. The pigmentation often has the appearance of dark droplets within the lesion, as seen in this picture. Image courtesy Michael L. Ramsey, MD. View Full Size Image Picture Type: Photo Caption: Picture 11. Basal cell carcinoma of the skin. This infiltrating basal cell cancer has ill-defined borders and telangiectases. Image courtesy Michael L. Ramsey, MD. View Full Size Image Picture Type: Photo Caption: Picture 12. Basal cell carcinoma of the skin. Postoperative wound after Mohs micrographic surgery demonstrates extensive subclinical involvement typical of many infiltrating and morpheaform basal cell carcinomas. Image courtesy Michael L. Ramsey, MD. View Full Size Image Picture Type: Photo Caption: Picture 13. Basal cell carcinoma of the skin. Large scarlike morpheaform basal cell cancer. Image courtesy Michael L. Ramsey, MD. View Full Size Image Picture Type: Photo BIBLIOGRAPHY Section 10 of 10 Author Information Introduction Clinical Differentials Workup Treatment Follow-up Miscellaneous Pictures Bibliography American Joint Committee on Cancer: Manual for Staging of Cancer. JB Lippincott; 1992. Baker SR, Swanson NA, Grekin RC: An interdisciplinary approach to the management of basal cell carcinoma of the head and neck. J Dermatol Surg Oncol 1987 Oct; 13(10): 1095-106[Medline]. Gallagher RP, Hill GB, Bajdik CD, et al: Sunlight exposure, pigmentary factors, and risk of nonmelanocytic skin cancer & Basal cell carcinoma. Archives of Dermatology 1995; 131: 157-63. Geisse J, Caro I, Lindholm J: Imiquimod 5% cream for the treatment of superficial basal cell carcinoma: results from two phase III, randomized, vehiclecontrolled studies. Journal of the American Academy of Dermatology 2004; 50: 722-33.[Full Text]. Miller SJ: Biology of basal cell carcinoma (Part I). J Am Acad Dermatol 1991 Jan; 24(1): 1-13[Medline]. Pascal RR, Hobby LW, Lattes R, Crikelair GF: Prognosis of "incompletely excised" versus "completely excised" basal cell carcinoma. Plast Reconstr Surg 1968 Apr; 41(4): 328-32[Medline]. Shumack S, Robinson J, Kossard S, et al: Efficacy of topical 5% imiquimod cream for the treatment of nodular basal cell carcinoma: comparison of dosing regimens. Archives of Dermatology 2002; 138: 1165-71[Medline][Full Text]. Sober AJ: Diagnosis and management of skin cancer. Cancer 1983 Jun 15; 51(12 Suppl): 2448-52[Medline]. Swanson NA: Mohs surgery. Technique, indications, applications, and the future. Arch Dermatol 1983 Sep; 119(9): 761-73[Medline]. Swetter SM, Waddell BL, Vazquez MD: Increased effectiveness of targeted skin cancer screening in the Veterans Affairs population of northern California. Preventive medicine 2003; 36: 164-71[Medline][Full Text]. Weber RS, Miller MJ, Goepfert H: Basal and Squamous Cell Skin Cancers of the Head and Neck. Baltimore: Lippincott Williams & Wilkins; 1996:9-33. Skin Cancer: Basal Cell Carcinoma excerpt