Supplementary Figure Legends (doc 42K)
advertisement
")
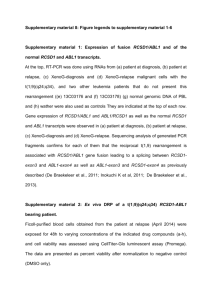
Supplementary Figure Legends IKZF1 deletions predict relapse in uniformly treated pediatric precursor B-ALL by Roland P. Kuiper et al. Supplementary Figure 1. Targeted copy number analysis using Multiplex Ligationdependent Probe Amplification (MLPA). A. Schematic representation of the IKZF1 gene with the position of the MLPA probes A-I (see Supplementary Table 6 for primer sequences). B. Representation of MLPA results of 20 patients of which six show intragenic deletions of exons 4-8 (case 6), exons 4-7 (case 9), exons 2-7 (case 26), exons 2-3 (case 34), and exons 2-8 (representing loss of entire locus in cases 24 and 28). In addition, case 12 shows a gain of control probe 4 (9q34.1) which is in agreement with the 7.6 Mb duplication of 9q34.12q34.3 observed by SNP array analysis. Supplementary Figure 2. Schematic overview of copy number variations in diagnosis and relapse samples of 34 pediatric precursor B-cell ALLs (vertical axis). Patients are ordered horizontally from early to late relapses (Tr), with two lanes representing the diagnosis and relapse sample, respectively. For cases 14, 21, 28, and 32 two subsequent relapse samples were analyzed. Copy number aberrations include bi-allelic loss (black), mono-allelic loss (red), single copy gain (light green), two-copy gain (green) and > two-copy gain (dark green). Supplementary Figure 3. Copy number intensities of an 0.4-Mb region on 7p12 encompassing the entire IKZF1 gene (NCBI human genome assembly hg18, chr7:50,078,258-50,490,342) in three diagnosis samples (Cases 6, 26, and 34) and one relapse sample (case 18) with focal IKZF1 deletions detected by high-density oligonucleotide arrays. Plots show the log2 ratios (y-axis) for 12,463 probes (x-axis) in 500-bps averaged windows. For each sample, deviations of probe log2 ratios from 0 are depicted by gray and black lines; those exceeding a threshold of 1.5 standard deviations from the mean probe ratio are depicted in green and red to represent relative gains and losses, respectively. The black bar in intron 3 of the IKZF1 gene indicates a sequence gap in the hg18 assembly and is not represented on the array. Supplementary Figure 4. Kaplan-Meyer estimates of Relapse-free survival (RFS) in a cohort of 116 precursor B-ALL patients (A), as well as in the subset of 25 patients that was enrolled in the ALL9 high-risk treatment group (B). This cohort was based on the unselected 1 cohort of 131 patients, but excludes all BCR-ABL1-postive cases (n=4) and all cases with an unknown BCR-ABL1 status (n=11). In each plot, curves are presented from the IKZF1 wildtype (black line) and IKZF1 deletion (dotted black line) cases. The data show that the association of IKZF1 deletion status with the occurrence of relapse remains significant in the total group, and shows a similar trend in the small HR treatment group. Follow-up for all patients is 8 years. Supplementary Figure 5. Schematic outline of the clonal relationship between diagnosis and relapse in childhood ALL according to three different models. In model A, relapses directly evolve from the major clone at diagnosis, which is compatible with those cases that show no changes in copy number abnormalities or show only acquired lesions (<32% of the relapses in the discovery cohort). In models B and C, relapses re-emerge from earlier (progenitor) cells (B) or from a minor sub-clone present at diagnosis (C), which can be associated with the absence of copy number abnormalities that were present at diagnosis, and appears to have 2