Curriculum Outcomes
advertisement

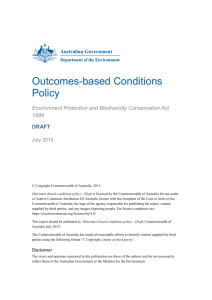
PAPER 08/CE/45 A REVISED STRUCTURE FOR THE EDINBURGH MBChB CURRICULUM BASED ON LEARNING OUTCOMES Outcomes-based education Outcomes-based education is an approach which has gained acceptance in medical education in recent years. It starts by defining the curriculum Outcomes at the time of graduation. These Outcomes are defined to match the requirements of medical clinical practice. The curriculum is then aligned to support students in achieving these Outcomes. There are many advantages to such an approach, but perhaps the main one is that students, graduates, employers (the National Health Service), patients and society have a much clearer statement of what they can expect from medical graduates entering the workplace. Medical schools are then accountable for the degree to which those expectations are met. An entire issue of “Medical Teacher” was devoted to outcomes-based education in 2007 – Vol 29, issue 7. For an overview see Harden RM. Outcome-based education; the future is today. Medical Teacher, 2007; 29: 625-629. Fig 1. A model for an outcomes-based curriculum Important questions for a medical school which aspires to an outcomes-based approach are : Is there a clear statement of the learning outcomes? Are these communicated effectively to staff and students and recognised by them? Is the course content explicitly and clearly aligned with the outcomes? Are the educational strategies, educational environment and learning opportunities chosen to support achievement of the outcomes? Is the strategy and structure for assessment and student progression explicitly and clearly aligned with the outcomes? Is student selection informed by the outcomes? How are the outcomes decided? Graduating outcomes for a UK medical curriculum can be subject to various influences: Discussion and negotiation within the Medical School and with NHS partners The guidance to medical schools from the General Medical Council, "Tomorrow's Doctors" (2009). The GMC inspects medical schools regularly to establish whether they are following this guidance. The 2009 version for the first time contains an explicit, multi-level Outcomes framework, which has been subjected to very extensive discussion, review and consultation. “The Scottish Doctor – a competent and reflective practitioner” – published by the Scottish Deans Medical Education Group after a national consultation process (2002). Has been very influential world-wide as a model for such approaches. “The Tuning Project (Medicine) – learning outcomes/competences for undergraduate medical education in Europe” – a consensus statement, based on a Europe-wide survey funded by the European Commission, published by the University of Edinburgh (2008). Currently the basis of ongoing work on curriculum harmonisation in support of the mandatory mutual recognition of medical degrees in Europe. There is a growing consensus about the essential outcomes of primary medical degrees and how they are best described and presented, and there is already considerable convergence between these different influences. Proposal to CAFMG It is proposed that the Edinburgh curriculum is now structured and described in terms of the curriculum Outcomes, and its assessment strategy and framework aligned with that change. Since the medical school will be accountable for the achievement of the GMC “Tomorrow’s Doctors” outcomes by all its graduates, and will required in future years to show evidence of this, it seems strategically desirable to use those outcomes as the primary basis for the new structure - albeit with appropriate adjustments and additions to reflect the particular nature and character of the Edinburgh graduate. TD 2009 specifies 15 major curriculum Outcomes. Experience suggests that this is quite a large number to manage effectively at curriculum level. A very simple adjustment, as shown below (Table 1) reduces the number to 12, and makes alignment with the current Edinburgh structure, the Scottish Doctor, and the Tuning Project more straightforward. Outcomes as the end-product of curriculum Themes A simple and logical approach to linking curriculum content to the outcomes is to say that each Outcome is supported by an Outcome Theme. These Themes then encompass the teaching, learning and assessment in all five years of the curriculum. Each Theme has an identified Theme Head, supported by a team of staff active in this area. The assessments related to each Theme accumulate and allow us to be sure that graduates, at the time of graduation, have been adequately assessed in each of the Outcomes. Level 2 outcomes All existing outcome frameworks have some degree of hierarchical structure, usually referred to as Levels. These are not defined in terms of the importance of the outcomes, but rather the level of detailed specification, and to some degree, their scope and dimensions. This can be a source of confusion – e.g. in the “Scottish Doctor”, the major outcomes are referred to as Level 2. TD 2009 has an “overarching outcome” which could be said to be Level 1, then three subdivisions which could be Level 2, before the major outcomes. It is proposed that for simplicity, the Edinburgh “major Outcomes” are referred to as Level 1. A series of more detailed Level 2 Outcomes would be mapped under each Level 1 Outcome. Obviously this process cannot be undertaken in detail until the Level 1 structure is agreed, but would be a key task for the coming academic year. PVTs and KCTs An important question is how to deal with areas of learning that were separately identified in our previous curriculum structure as “Portfolio Vertical Themes” or “Key Clinical Topics”, but which would not figure overtly in the Level 1 outcomes. Examples include pain, disability, nutrition, life cycle, and clinical conditions such as diabetes. Other than the rather vague label of “topic” (“a general consideration suitable for argument… a matter”: Chambers Dictionary) , there is no single descriptive term that will fit all of these conceptually. Pain is primarily a symptom, life cycle is a concept, diabetes is a disease. However, it is reasonably straightforward to define them in terms of the learning outcomes to be achieved – e.g. the ability to manage pain effectively; understanding of the influence of the life cycle on human health and disease; ability to investigate, diagnose and manage patients with diabetes. It is proposed that these areas of learning are redefined as Level 2 Outcomes and mapped to a Level 1 Outcome/Theme. Clearly they do not all fit neatly under a single Level 1 Outcome and there is inevitably some degree of empiricism involved. In practice however, the important thing is that these areas are clearly identified, and that students learn about them and are assessed – not necessarily the detail of where exactly they are placed in the Outcomes framework. Similarly, such a process should not be interpreted as diminishing the perceived importance of these areas of learning. At this stage the particular emphasis and character of the Edinburgh curriculum can be reflected in the formulation of the Level 2 outcomes. The Portfolio would have to move to a slightly less specific remit – effectively it would be a tool for learning and assessment about any and all of the Outcomes, but with a focus on those which lend themselves particularly to portfolio-based learning. Such a structure has already been outlined by Dr Helen Cameron. Blueprinting of Assessments Blueprinting is the process by which the content of an integrated examination is mapped on a matrix grid against the Outcomes. This allows us to track the assessment of students over time under each Outcome, and therefore allows us to assure the General Medical Council that our graduates have been adequately assessed in each outcome at the time of graduation. This, in turn, allows the General Medical Council to enter graduates on the Medical Register and provide them with a provisional license to practise. Learning objectives Learning objectives define discrete items of teaching, learning and assessment for the various components of the course – e.g. a lecture, module, or attachment. They can be viewed as the building blocks of the Outcome Themes, provided they have been explicitly mapped against the Outcome Themes. This is currently being undertaken as part of the OPAL Project, but cannot be finalised until the new curriculum structure is confirmed. In such a model, every learning objective relates to a learning opportunity, module or attachment, but at the same time is a building block of an Outcome Theme, contributing to achievement of a graduating Outcome. Table 1. Proposed Edinburgh Level 1 outcomes, with corresponding TD 2009 statements. EDINBURGH MBChB LEVEL 1 OUTCOMES GMC TOMORROW’S DOCTORS 2009 OVERARCHING OUTCOME An Edinburgh medical graduate will be a caring, competent, confident, ethical and reflective practitioner, equipped for high personal and professional achievement, able to provide leadership and to analyse complex and uncertain situations. GMC150. Medical graduates are tomorrow’s doctors. In accordance with Good Medical Practice, they must make the care of patients their first concern, applying their knowledge and skills in a competent and ethical manner, using their ability to provide leadership and to analyse complex and uncertain situations. THE DOCTOR AS SCHOLAR AND SCIENTIST 1. BIOMEDICAL AND CLINICAL SCIENCES GMC152. Apply to medical practice the biomedical scientific principles, method and knowledge of: anatomy, biochemistry, cell biology, genetics, immunology, microbiology, molecular biology, nutrition, pathology, pharmacology and physiology. 2. PSYCHOLOGICAL ASPECTS OF MEDICINE GMC153. Apply psychological and social principles, method and knowledge to medical practice. 3. SOCIAL SCIENCES AND PUBLIC HEALTH Social sciences part of GMC153, but in Edinburgh clearly part of Outcome 3. GMC154. Apply to medical practice the principles, method and knowledge of population health and the improvement of health and health care. 4. EVIDENCE-BASED MEDICINE AND RESEARCH GMC 155. Apply scientific method and approaches to medical research. THE DOCTOR AS PRACTITIONER 5. CONSULTING WITH A PATIENT GMC 157. Carry out a consultation with a patient. 6. CLINICAL PRESENTATIONS, DIAGNOSIS AND MANAGEMENT GMC 158. Diagnose and manage clinical presentations. 7. CLINICAL COMMUNICATION GMC159. Communicate effectively with patients and colleagues in a medical context. 8. EMERGENCY CARE, FIRST AID, RESUSCITATION AND PRACTICAL PROCEDURES GMC160. Provide immediate care in medical emergencies, including first aid and resuscitation. 9. PHARMACOLOGY AND THERAPEUTICS GMC161. Prescribe drugs safely, effectively and economically. 10. MEDICAL INFORMATICS GMC 163. Use information effectively in a medical context. THE DOCTOR AS PROFESSIONAL 11. MEDICAL ETHICS, LEGAL AND PROFESSIONAL RESPONSIBILITIES GMC165. Behave according to ethical and legal principles. 12. PERSONAL AND PROFESSIONAL DEVELOPMENT GMC166. Reflect, learn and teach others. GMC167. Learn and work effectively within a multi-professional team. GMC168. Protect patients and improve care. Professor Allan Cumming Director of Undergraduate Learning and Teaching, CMVM 29/07/09