Chapter 13, The Respiratory System
advertisement

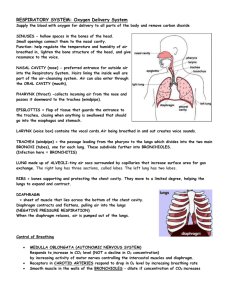
The Respiratory System – Notes Part I Why do we breathe? “To live? Because our lungs need it? Because it is vital to life?” Yes, but why? The correct answer is, “for aerobic respiration.” Oxygen is the final electron acceptor in the electron transport chain (ETC). But what is Aerobic Respiration? It is the process that the cells use to break down glucose for energy. Aerobic respiration: C6H12O6 + 6 O2 → 6 CO2 + 6 H2O + 34 ATP During aerobic respiration, which occurs in all of our cells, glucose is broken down for its energy. Oxygen is the final electron acceptor in the electron transport chain (ETC) which is the final step of aerobic respiration. At the end of the ETC, one molecule of oxygen combines with two electrons and two hydrogen atoms to form water. When the ETC is functioning properly with oxygen available, the electrons of the ETC produce 34 ATP per glucose molecule. (This is a large amount of energy.) Without ATP, the cells of the body would not function. Therefore, without oxygen, ATP can only be produced in small amounts which are not sufficient to support life. Lactic acid fermentation (no oxygen available): C6H12O6 → + 2 C3H6O3 + 2 ATP http://highered.mcgrawhill.com/sites/dl/free/007250747 0/234439/mc_ch25_fig10.jpg March 25, 2009 Importance of the Respiratory System: The cardiovascular system and respiratory system have a shared responsibility to supply the body with oxygen and rid it of carbon dioxide. The cardiovascular system and lymphatic system combined are sometimes called the circulatory system. 1 Organs of the Respiratory System: Nasal cavity, pharynx, larynx, trachea, bronchi and their smaller branches, and the lungs which serve to purify (of dust and bacteria), humidify, warm, and transport oxygen to and carbon dioxide from the bloodstream. The Nasal Cavity Nose – contains the external nares (anterior naris) or nostrils that allow air to enter Nasal Cavity – The nasal cavity is lined with a ciliated mucosa (a mucus membrane containing cells with tiny hairs) overlaying a blood-rich connective tissue layer (nose bleeds). The blood is used to warm the air. The mucus moistens the air, traps bacteria, and traps dust as the air passes by. In addition the cilia (tiny hairs) are able to push the mucus toward the pharynx where it is swallowed. http://content.answers.com/main/cont ent/img/elsevier/dental/f0098-01.jpg March 25, 2009 The nasal cavity is divided by a midline of tissue called the nasal septum. Three conchae bones can be found on the walls of the nasal cavity to increase the surface area of the mucosa. Olfactory receptors – located near the cribiform plates of the Ethmoid bone which is located on the superior surface of the nasal cavity. Hard Palate – surface of the mouth supported by bone that separates the nasal cavity from the oral cavity 2 Soft Palate – also located on the surface of the oral cavity, but is not supported by bone Paranasal Sinuses – found within the frontal, sphenoid, ethmoid, and maxillary bones surrounding the nasal cavity; produce mucus which drains into the nasal cavity and is removed by nose blowing http://www.sinuscure.com.au/nasanat.htm March 25, 2009 The Pharynx: Pharynx (throat) – a muscular passageway about 13cm long that functions as a passageway for air and food. From the pharynx, air enters the larynx, where as food goes into the esophagus. Clusters of lymphatic tissue (fight infection) called tonsils are found in the pharynx. o The pharyngeal tonsils (adenoids) are located in the superior portion of the larynx. o The palatine tonsils are located at the end of the soft palate o The lingual tonsils are located at the base of the tongue. 1 Pharyngeal tonsil 2 Palatine tonsil 3 Lingual tonsil 4 Epiglottis Inflammation of the tonsils (tonsillitis) blocks air flow to nose and restricts it to the mouth. Previously treated by removing tonsils, tonsillitis is now typically treated with antibiotics. http://nwmc.discoveryhospital.com /encyclopedia/Images/Ent-41.jpg March 25, 2009 3 The Larynx: Larynx (voicebox) – located inferior to the pharynx, formed by eight rigid hyaline cartilages, and a flap of elastic cartilage (epiglottis). The largest ridge of hyaline cartilage is the thyroid cartilage (Adam’s apple). http://www.cancerhelp.org.uk/canc er_images/Larynx.gif March 25, 2009 Epiglottis The epiglottis is responsible for directing food and water into the esophagus and air into the trachea. A cough results when food or water enter the trachea. Part of the mucous membrane of the larynx forms a pair of folds called the vocal cords which vibrate with expelled air. The slit-like passage between the vocal cords is the glottis. http://www.yoursurgery.com/proce dures/laryngectomy/images/Vocal CordAnat.jpg March 25, 2009 Glottis The Trachea: Trachea (windpipe) – located inferior to the larynx (about 10-12 cm long) and travels to the right and left primary bronchi. The trachea is lined with ciliated mucosa. The cilia beat upward in order to remove debris so that it too may be swallowed. Smoking creates too much mucus which eventually kills the cilia and leaves coughing as the only means to cleanse the trachea. C-shaped rings of hyaline cartilage support the trachea and do not allow it too collapse in on itself. The open part of the “C” also allows us to swallow large parts of food by folding inward allowing more room for the esophagus within the neck. 4 Heimlich maneuver – used to remove an obstruction that has closed off the airways (trachea) Tracheostomy/ Tracheotomy – surgical opening in the trachea to provide an alternate route for air to pass http://www.swankpets.com/images /Trachea%20anatomy.jpg March 25, 2009 The Lungs: Lungs – large organs that occupy most of the thoracic cavity 5 Mediastinum – occupies the remainder (center) of the thoracic cavity and includes the heart, great blood vessels, bronchi, and esophagus Pulmonary (Visceral) Pleura – a type of serous membrane that lines the outside of each lung Parietal Pleura – a type of serous membrane that lines the walls of the thoracic cavity. Together the parietal and visceral pleura secrete serous fluid (pleural fluid) that lubricates the two membranes, reducing friction and allowing the lungs to slide past one another and to glide along the thoracic walls. http://dic.academic.ru/pictures/enw iki/77/Mediastinum_anatomy.jpg March 25, 2009 Apex of lung – narrow superior portion of each lung located just deep to the clavicle Base of lung – broad inferior portion of each lung that rests on the diaphragm Note: In humans, the left lung has two lobes and the right lung has three lobes http://academic.kellogg.cc.mi.us/he rbrandsonc/bio201_McKinley/f2512a_gross_anatomy_o_c.jpg March 25, 2009 6 Airway passages: Primary Bronchi – right and left divisions of the trachea that continue to divide into smaller and smaller branches before reaching the bronchioles and finally the alveoli of the lungs Secondary Bronchi – branch off the primary bronchi and are smaller in diameter Tertiary Bronchi – branch off the secondary bronchi and are even smaller in diameter Bronchioles – smallest of the conducting passageway between the bronchi and the alveoli Alveoli (alveolar sacs) – terminal grape-shaped air sacs found within the lungs, located at the end of the bronchioles, where gas exchange occurs between the lungs and the blood; compose the bulk of the lungs http://www.cartage.org.lb/en/theme s/Sciences/LifeScience/GeneralBio logy/Physiology/RespiratorySyste m/HumanRespiratory/HumanRespi ratory.htm March 25, 2009 The Respiratory Membrane (air-blood barrier) – composed of thin simple squamous epithelial of the alveoli and a “cobweb” of pulmonary capillaries that allows gas exchange to occur by simple diffusion (Oxygen into the blood and Carbon Dioxide out of the blood) The surface area provided for gas exchange in a healthy individual is 70 to 80 square meters. Bigger than the surface area of the floor in our classroom! Macrophages – the last line of defense within the lungs; phagocytotic cells that are capable of consuming bacteria, carbon particles, and debris within the alveoli Cuboidal cells – larger cells that are found within the simple squamous epithelial cells of the alveoli – these cells secrete surfactant that coats the alveoli and is important in lung function lowers the surface tension of the film of water lining each alveolar sac so that the alveoli do not collapse between each breath Premature babies may not have cells that make enough surfactant until they mature a bit more. This is why premature babies needs to be on respirators. 7 The Respiratory System – Notes Part II Respiratory Physiology: The process of Respiration 4 Parts to Respiration: 1. Pulmonary Ventilation (breathing) – air must move in and out of the lungs 2. External Respiration – oxygen must enter the blood from the alveoli and carbon dioxide must leave to blood and enter the alveoli 3. Respiratory Gas Transport – blood must carry the respiratory gases between the lungs and the tissues of the body 4. Internal Respiration - oxygen must enter the cells from the blood and carbon dioxide must leave the cells and enter the blood in order to be transported back to the lungs Mechanisms of Pulmonary Ventilation / Breathing (Page 383) Inspiration – air is flowing into the lungs Expiration – air is flowing out of the lungs 1. Process of Inspiration: As the diaphragm contracts it moves inferiorly and flattens. At the same time the intercostal muscles contract lifting the rib cage. The lungs must follow the diaphragm and the thoracic walls because they are connected by the pleural membrane. This increases the size of each lung (increasing intrapulmonary volume) and decreases intrapulmonary pressure causing a vacuum which draws air into the lungs. 2. Process of Expiration: The process of expiration is a passive process in which the diaphragm and the external intercostal muscles relax, compressing the lungs, causing the intrapulmonary pressure to exceed atmospheric pressure. The air within the lungs then flows out to equalize the pressure. During exercise, we breathe more deeply and at a faster rate. At this time expiration becomes an active process. Various chest and abdominal muscles capable of lowering the ribs may be used to aid in expiration. (Various diseases of the lung may also require the person to use active expiration as well.) 8 External Respiration, Gas Transport, and Internal Respiration Respiratory Gases / Partial Pressures What causes carbon dioxide to move out of the body and oxygen to move in? http://www.octc.kctcs.edu/GCap lan/anat2/notes/Image247.gif March 25, 2009 Oxygen transportation: Oxygen is transported in the blood in two ways: Most attaches to hemoglobin in the RBCs to form oxyhemoglobin (HbO2) The remaining small amount of oxygen is transported in the plasma (fluid of blood) During internal respiration, oxygen leaves the blood and diffuses into the tissues. Carbon dioxide transportation: During internal respiration, carbon dioxide diffuses into the blood from the tissues and combines with water to form carbonic acid which quickly splits into hydrogen ions and bicarbonate ions CO2 + H2O ↔ H2CO3 ↔ H+ + HCO3Most carbon dioxide is transported in the plasma as bicarbonate ion (HCO3-) The remaining 20-30% is carried inside the RBCs attached to a different site than oxygen 9 External respiration: In order for carbon dioxide to be released into the alveoli, HCO3must first combine with hydrogen (H+) to form carbonic acid (H2CO3) which is quickly split into water and carbon dioxide. The carbon dioxide then diffuses into the alveoli from the blood stream. Relationship between carbon dioxide and pH The pH of blood decreases (= becomes more acidic) when more carbon dioxide is present. This is due to increased levels of carbonic acid and subsequently hydrogen and bicarbonate ions. The body responds to pH levels by increasing or decreasing respiration rates, driving the equation above either towards the carbon dioxide side to increase pH or towards the bicarbonate side to decrease pH. Hypoventilation – slow or shallow breathing that increases carbonic acid (carbon dioxide) and may lead to acidosis (homeostasis is disrupted because body fluids are too acidic) Hyperventilation – fast, deep breathing that decreases carbonic acid (carbon dioxide) and may lead to alkalosis (homeostasis is disrupted because body fluids are too basic) Breathing into a paper bag during hyperventilation reduces the amount of carbon dioxide you will be able to get rid of and decreases the chances of alkalosis Respiratory Rates, Volumes, and Capacities Respiratory rates throughout life: o In the fetus the lungs are filled with fluid and all respiratory exchanges are made though the placenta. o 40-80 respirations per minute in newborns o 30 respirations per minute in infants o 25 respirations per minute at 5 years old o 12-15 respirations per minute in adults o Increasing respirations per minute in old age Control of Respiratory Rate 1. The diaphragm and the intercostals are regulated by the phrenic and intercostal nerves respectively. The control centers for these nerves are located in the medulla and Pons. 2. Rate of respiration can be modified by physical, emotional, and chemical factors o Physical Factors: demand for more oxygen or removal of carbon dioxide o Emotional Factors: being scared or frightened increases respiration 10 http://www.scottsdalecc.edu/ricker/psy101/ readings/section_1/images/brainstem.jpg March 25, 2009 o Chemical Factors: change in pH levels in the blood o Consciously controlling breathing = Volition on breathing: one can only hold their breath for only so long before the unconscious control takes over Respiratory capacity o Respiratory capacity is regulated by size, sex, age, and physical condition o Average lung capacity of a healthy adult is 6 liters or 6000 ml 1. Tidal Volume – is referred to as the amount of air transferred in one normal resting breath (500 ml or 1 pint) 2. Inspiratory Reserve Volume (IRV) – the amount of air that can be taken in forcibly over the tidal volume (2100 – 3100ml) 3. Expiratory Reserve Volume (ERV) – the amount of air that can be forcibly exhaled after a tidal expiration (1000ml) 4. Residual Volume – the amount of air that remains after the ERV is exhaled; air that is always present allowing gas exchange to continue uninterrupted (1100ml) 5. Vital Capacity (TV + IRV + ERV) – the total amount of exchangeable air (4500ml) 6. Dead Space Volume – air within the conducting respiratory passageways (150ml) 7. Functional Volume – air that actually reaches the respiratory zone and contributes to gas exchange 11 Respiratory Conditions and Disorders Hypoxia A condition in which inadequate oxygen is available to tissue (increases with old age, anxiety, asthma, and other respiratory diseases) Carbon Monoxide Poisoning Carbon monoxide (CO) binds to hemoglobin at the same site as oxygen usually does and competes vigorously for those binding sites Chronic obstructive pulmonary diseases (COPD) – a series of diseases including chronic bronchitis and emphysema, commonly brought on by smoking, leading to coughing and frequent pulmonary infections and ultimately respiratory failure Emphysema – the alveoli enlarge as the walls of adjacent chambers break through and chronic inflammation promotes fibrosis (scarring) of the lungs. The process of exhalation must become active instead of passive (the person must work to breathe out) and since oxygen is always left in large amounts in the lungs, results in cyanosis (deficient oxygenation of the blood) Chronic Bronchitis – the mucosa of the lower respiratory passages become severely inflamed and produces excessive amounts of mucus impairing both ventilation and gas exchange and increasing the likelihood of infection Lung Cancer – accounts for 1/3 of all cancer deaths in the U.S. (90% of patients are smokers) Due to the effects of chemicals in cigarettes, the nasal hairs, mucous glands, and cilia which protect the lungs become overwhelmed. Cigarettes also depress the activity of lung macrophages (WBCs). Finally, the 15 or so carcinogenic chemicals in cigarettes enter the lungs and translate into lung cancer by causing the mucosal cells to mutate and divide rapidly Squamous cell carcinoma (20-40% of cases) – arises in the epithelium of the larger bronchi and tends to form masses that hollow out and bleed Adenocarcinoma – (25-35% of cases) – originates in the peripheral areas of the lungs as solitary nodules that develop from bronchial mucous glands and alveolar epithelial cells Small cell carcinoma (10-20% of cases) & Oat Cell Carcinoma – consist of lymphocyte-like epithelial cells that originate in the primary bronchi and grow aggressively in cords or small grape-like clusters within the mediastinum. Treatment – removal of diseased lung, radiation, and chemotherapy. The overall 5 year survival rate is only 7% and the average person survives only 9 months after diagnosis. Pneumonia bacterial or viral infection in the lungs. Pneumonia causes the alveoli to become filled with fluid which interferes with the process of external respiration. The bronchioles are often also affected by the infection as well. Asthma is a chronic condition in which the airways spasm and narrow and may even become inflammed. Because the airways are narrowed, the ability to bring air in and out of the lung becomes difficult. Atelectasis (collapsed lung) – results when the pressure within the pleural space (which is always negative) becomes equal to the atmospheric pressure 12