This Article Abstract Figures Only Full Text (PDF) Submit a
advertisement
 Submit a")
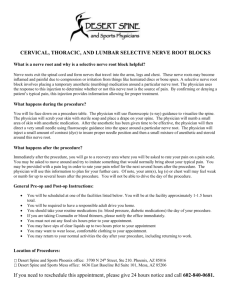
(Radiology. 2001;219:811-816.) © RSNA, 2001 This Article Abstract Figures Only Musculoskeletal Imaging Full Text (PDF) Submit a response Radial Nerve Palsy Associated with Humeral Shaft Fracture: Evaluation with US—Initial Experience1 Alert me when this article is cited Alert me when eLetters are posted Alert me if a correction is posted Citation Map Services Email this article to a friend Gerd Bodner, MD, Wolfgang Buchberger, MD, Michael Schocke, MD, Reto Bale, MD, Burkart Huber, MD, Christoph Harpf, MD, Eva Gassner, MD and Werner Jaschke, MD 1 From the Departments of Radiology (G.B., W.B., M.S., R.B., E.G., W.J.), Traumatology (B.H.), and Plastic Surgery (C.H.), University Hospital of Innsbruck, Anichstrasse 35, 6020 Innsbruck, Austria. Received January 18, 2000; revision requested March 7; final revision received November 2; accepted November 9. Address correspondence to G.B. (email: gerd.bodner@uibk.ac.at). Similar articles in this journal Similar articles in PubMed Alert me to new issues of the journal Download to citation manager Cited by other online articles Google Scholar Articles by Bodner, G. Articles by Jaschke, W. Articles citing this Article PubMed PubMed Citation Articles by Bodner, G. Articles by Jaschke, W. TOP ABSTRACT INTRODUCTION MATERIALS AND METHODS RESULTS DISCUSSION REFERENCES ABSTRACT PURPOSE: To determine the feasibility of using ultrasonography (US) for evaluation of a radial nerve injury associated with humeral shaft fracture. MATERIALS AND METHODS: In a prospective study, 11 consecutive patients with sensorimotor radial deficiency after distal humeral fracture were evaluated with conventional radiography, US, electroneurography, and electromyography. Surgical repair of the fracture and nerve inspection were performed in five patients. The remaining six patients were successfully treated conservatively. The US appearance of the radial nerve was studied in 10 healthy volunteers and in the noninjured arm of the 11 patients for comparison. RESULTS: In five patients, US findings of a severely damaged radial nerve were confirmed at surgical nerve inspection. In one patient, the nerve was entrapped between fragments. One patient had a complete nerve dissection, one had a lacerated nerve from a loose compression plate, and one had a nerve riding on the edge of a bone fragment. In the fifth patient who underwent surgical inspection, the nerve was buried in the callus. In the six patients treated conservatively, US showed continuity of the nerve. CONCLUSION: US may be useful for accurate evaluation of the radial nerve in patients with nerve palsy associated with humeral shaft fracture. Index terms: Humerus, fractures, 416.411, 416.413 • Nerves, peripheral, 416.43 • Nervous system, US, 416.12989 • Ultrasound (US), utilization, 416.12989 TOP ABSTRACT INTRODUCTION MATERIALS AND METHODS RESULTS DISCUSSION REFERENCES INTRODUCTION Radial nerve injuries associated with fractures of the humerus are the most common traumatic nerve lesions in long-bone fractures. The overall prevalence of these injuries has been reported to be 2%–18% of all patients with fractures of the humeral shaft (1– 10). Owing to the close anatomic relationship of the radial nerve with the bone (Fig 1) as the nerve courses through the middle and distal thirds of the upper arm and because of the diminished mobility of the nerve where it pierces the lateral intermuscular septum, fractures with associated radial nerve palsy are usually localized to the middle and distal thirds of the humerus (1–19). The nerve may be injured by direct contusion or laceration, by fracture fragments, by interposition between fragments, or by traction when the bone ends are forcibly separated. Iatrogenic damage to the radial nerve may occur during closed or open reposition, for example, following internal fixation of the fracture with a compression plate (2,6). Figure 1. Diagram shows the close relationship of the radial nerve (RN) to the humerus at the spiral groove. The nerve is accompanied by the deep brachial artery (DBA), which arises from the brachial artery (BA). Sections marked Fig 2a-2c correspond to the US images in Figure 2a-2c. View larger version (26K): [in this window] [in a new window] A review of the literature shows that the proper treatment for fractures of the humerus complicated by paralysis of the radial nerve is still under debate. Spontaneous recovery of nerve function has been reported to occur in 73%–92% of cases (7,10,11). Therefore, many authors prefer primarily conservative management with close electromyographic follow-up and recommend surgical exploration only if the nerve shows no signs of recovery within 3–4 months (1,7,9–11). However, spontaneous recovery is unlikely to occur if the radial nerve is lacerated, riding on or pinched in between bone fragments, or entrapped in callus or scars (3,4,7,8,10,13–15,17,19). During the past decade, ultrasonography (US) has become an important diagnostic tool in musculoskeletal radiology. Because of major improvements in spatial and contrast resolution with high-frequency probes, imaging of small soft-tissue structures, including peripheral nerves, has become feasible (19–25). Recently, we reported a case of a US-detected radial nerve entrapment between fragments in a patient with a fragmented humeral shaft fracture (19). This observation prompted us to perform this prospective study to assess the accuracy of US for identification of the cause of radial nerve paralysis associated with humeral fractures. MATERIALS AND METHODS TOP Normal Regional and US Anatomy ABSTRACT The radial nerve is the largest branch of the posterior INTRODUCTION MATERIALS AND METHODS cord of the brachial plexus and contains cervical root RESULTS contributions from C5 through C8. It consists of five DISCUSSION to eight fascicles with motor and sensory components REFERENCES that supply the muscles of the extensor compartments (ie, the triceps muscle, the lateral part of the brachialis muscle, the brachioradialis muscle, the forearm extensors, the overlying skin of the forearm, and the dorsolateral area of the hand). At US, the radial nerve appears as a hyperechoic structure with parallel linear echoes on a longitudinal scan and as an oval or round structure with hypoechoic areas, corresponding to the nerve fascicles, on a transverse scan. It can be best identified at the posterior and lateral aspect of the humeral shaft, where the nerve runs alongside the brachial artery, first between the coracobrachialis and teres major muscles and then between the muscle bellies of the medial and lateral heads of the triceps muscle (Fig 2a, 2b). Approximately 10 cm proximal to the lateral epicondyle of the humerus, the radial nerve penetrates the lateral intermuscular septum and enters the anterior space of the upper arm, where it lies volar to the brachialis muscle and dorsal to the brachioradialis muscle (Fig 2c). Just anterior to the lateral epicondyle, the nerve bifurcates into the sensory (or superficial branch of the radial nerve) and the motor (or deep branch of the radial nerve and posterior interosseous nerve) components. Figure 2a. Transverse US images obtained with power Doppler mode in a 39-year-old male volunteer. Images a-c correspond to the upper, middle, and lower thirds, respectively, of the humerus in the diagram in (a) At the proximal third of the right humerus (H), the radial nerve (straight arrow) is accompanied by the deep brachial artery (curved arrow), which arises from the brachial artery (BA). The radial nerve lies between the coracobrachialis muscle (CB) and the teres major muscle (TM). (b) At the View larger version (167K): middle third of the humerus (H), the radial [in this window] nerve (straight arrow) is adjacent to the bone in [in a new window] the spiral groove and is accompanied by the deep brachial artery (curved arrow). LTM = lateral head of the triceps muscle, MTM = medial head of the triceps muscle. (c) At the distal third of the humerus (H), the radial nerve (arrow) lies between the brachioradialis muscle (BRM) and the brachialis muscle (BM). Figure 2b. Transverse US images obtained with power Doppler mode in a 39-year-old male volunteer. Images a-c correspond to the upper, middle, and lower thirds, respectively, of the humerus in the diagram in Figure 1. (a) At the proximal third of the right humerus (H), the radial nerve (straight arrow) is accompanied by the deep brachial artery (curved arrow), which arises from the brachial artery (BA). The radial nerve lies between the coracobrachialis muscle (CB) and the teres major muscle (TM). (b) At View larger version (173K): the middle third of the humerus (H), the radial [in this window] nerve (straight arrow) is adjacent to the bone in [in a new window] the spiral groove and is accompanied by the deep brachial artery (curved arrow). LTM = lateral head of the triceps muscle, MTM = medial head of the triceps muscle. (c) At the distal third of the humerus (H), the radial nerve (arrow) lies between the brachioradialis muscle (BRM) and the brachialis muscle (BM). Figure 2c. Transverse US images obtained with power Doppler mode in a 39-year-old male volunteer. Images a-c correspond to the upper, middle, and lower thirds, respectively, of the humerus in the diagram in Figure 1. (a) At the proximal third of the right humerus (H), the radial nerve (straight arrow) is accompanied by the deep brachial artery (curved arrow), which arises from the brachial artery (BA). The radial nerve lies between the coracobrachialis muscle (CB) and the teres major muscle (TM). (b) At View larger version (137K): the middle third of the humerus (H), the radial [in this window] nerve (straight arrow) is adjacent to the bone in [in a new window] the spiral groove and is accompanied by the deep brachial artery (curved arrow). LTM = lateral head of the triceps muscle, MTM = medial head of the triceps muscle. (c) At the distal third of the humerus (H), the radial nerve (arrow) lies between the brachioradialis muscle (BRM) and the brachialis muscle (BM). US Technique With the subjects in a supine position, US was performed (HDI 5000; Advanced Technology Laboratories, Bothell, Wash) with use of a 5–12-MHz broadband lineararray probe. The elbow was flexed at 90° and positioned on a cushion to allow US access to the lateral part of the humerus. The radial nerve was identified at the proximal part of the upper arm and was followed distally to the lateral humeral epicondyle. The shape, echotexture, and integrity of the radial nerve were assessed. The coracobrachialis muscle, teres major muscle, triceps muscle, brachioradialis muscle, brachialis muscle, and deep brachial artery were used as landmarks to best identify the radial nerve at the posterior and lateral aspects of the humerus (Fig 2). On transverse US scans, the mediolateral and anteroposterior diameters of the nerve were measured at the proximal third of the humerus where the nerve is found between the coracobrachialis and teres major muscles, at the middle third where the nerve enters the spiral groove and lies between the medial and lateral heads of the triceps muscle, and at the distal third of the humerus where the nerve lies between the brachioradialis and brachialis muscles. Measurements were taken in both arms of the volunteers as well as in the injured and noninjured arm of the patients. For statistical analysis, the unpaired t test was performed to compare the mean diameter measurements of both arms of the volunteers with those of the noninjured arms of the patients. Also, the mean diameter measurements of the fractured arms were compared with those of the noninjured arms and control group. A P value less than .05 was considered to indicate a statistically significant difference. Patients In a prospective study from May 1998 through February 1999, 11 consecutive patients (seven male and four female patients; mean age, 38 years; range, 10–72 years) with complete or partial radial nerve paralysis following a fracture of the humeral shaft were examined with US. All patients had sustained severe trauma to the upper arm (car accident, n = 5; heavy machinery accident, n = 2; bicycle accident, n = 2; motorbike accident, n = 1; sailing accident, n = 1). Seven fractures were located at the right humerus and four at the left humerus. Seven fractures were located at the middle third of the humerus and four at the distal third. The fracture type was spiral in four patients, short oblique in three patients, transverse in two patients, and comminuted in two patients. The interval between the trauma and initial presentation to our department was 1–8 weeks (mean, 19 days). Nine patients had an acute fracture, and two had been treated with an internal fixation and compression plate. All patients underwent a thorough neurologic examination, including electroneurography, electromyography, and US examination of the injured and the contralateral noninjured arm, as described in the preceding section. In all patients, anteroposterior and lateral radiographs of the fractured humerus were available for comparison. Clinical follow-up was performed in nine of the 11 patients and combined with electrodiagnostic testing and US for a least 6 months or until complete functional recovery. At US examination, a possible nerve displacement by hematoma or compression by displaced fragments, extensive fracture hematoma, or callus was recorded. Integrity of the nerve was defined as continuity of the nerve fascicles on longitudinal US scans. A completely disrupted nerve was diagnosed if proximal and distal nerve stumps were found and a gap between the stumps could be demonstrated. Images were recorded on laser prints and stored electronically. Electroneurography and electromyography were performed in all patients to determine the degree of impairment of the radial nerve. The results of these tests were unknown to the radiologist at the time of US examination. Five patients subsequently underwent surgical nerve inspection. US findings were known to the surgeons at the time of surgery. Volunteers In addition to the patient studies, 10 healthy volunteers (five men and five women; mean age, 45 years; range, 34–56 years) were also examined with US by one radiologist (G.B.). The shape, echotexture, and course of the radial nerve along the humerus were assessed on transverse and longitudinal scans in both arms, and measurements were taken as described in the US Technique section. All patients and volunteers gave informed consent for the diagnostic procedures, and investigations were performed according to the Declaration of Helsinki principles (26). TOP ABSTRACT INTRODUCTION MATERIALS AND METHODS RESULTS DISCUSSION REFERENCES RESULTS Volunteers In the 10 healthy volunteers, the radial nerve could be identified by means of US in every case. Table 1 shows the diameters (anteroposterior and mediolateral) of the radial nerve measured at three different levels in both arms of the volunteers and in the noninjured arm of the patients. No statistically significant difference was found in the measurements of both arms of the volunteers compared with those of the noninjured arms of the patients (P < .5). On the transverse scans, the nerve appeared rounded at the proximal third of the humerus, oval at the middle third, and rounded again at the distal third of the humerus. View this TABLE 1. US Measurements of the Normal Radial Nerve at Different Levels in the Humerus of Both Arms of the Volunteers table: [in this and Noninjured Arm of the Patients window] [in a new window] Patients with Radial Nerve Palsy In all 11 patients with posttraumatic radial nerve palsy, the radial nerve could be readily identified at US. Clinical information, electrodiagnostic findings, US findings, and the results of surgical exploration are summarized in Table 2. View this table: [in this window] [in a new window] TABLE 2. Test and Surgical Findings in 11 Patients with Radial Nerve Palsy Associated with Humeral Fracture In the five patients who underwent surgical nerve exploration, the US findings could be confirmed at surgery: In one patient with a humeral fracture (patient 1) who developed a complete motor and sensory radial nerve palsy, the radial nerve appeared markedly thinned and pinched between dislocated bone fragments at US. Proximal to the site of entrapment, the nerve showed hypoechoic fascicles that suggested diffuse nerve swelling. Surgical nerve inspection confirmed the US findings. In the second patient (patient 3), who sustained a fracture of the distal third of his left humerus with complete radial nerve paralysis, US showed complete disruption of the radial nerve, with a gap of approximately 5 cm. The proximal stump of the nerve showed extensive bulbous swelling (Fig 3a), which suggested amputation neuroma. The distal stump was markedly smaller (Fig 3b). Surgical reexploration confirmed complete laceration of the radial nerve (Fig 3c, 3d). The third patient (patient 7) had developed a progressive radial nerve paralysis after internal fixation with a compression plate. At US, the radial nerve appeared markedly flattened and stretched over the compression plate and enlarged proximally to the site of injury (Fig 4a). Surgical exploration confirmed dislocation of the plate, thinning and swelling of the radial nerve (which was surrounded by extensive scar tissue), and riding of the nerve on the detached proximal end of the plate (Fig 4b). The fourth patient (patient 9) had developed a radial nerve paralysis with complete motor and sensory deficit 24 hours after her arm was put in a cast. US showed a thickened radial nerve that was riding on the edge of a displaced fracture fragment. In the fifth patient (patient 11), who had progressively complete motor deficiency, US revealed a radial nerve buried into callus. Figure 3a. Spiral fracture in an 18-year-old man (patient 3) who had complete motor and sensory paralysis. (a) Longitudinal US scan shows a hypoechoic enlarged radial nerve (solid arrows) with bulbous swelling at the disrupted proximal part (open arrow). (b) Longitudinal US scan shows a hypoechoic distal nerve stump (solid arrow) 5 cm distal to the proximal stump; the View larger version (132K): distal part of the nerve has a normal, [in this window] hyperechoic appearance (open arrow). (c) [in a new window] Intraoperative photograph shows a proximal amputation neuroma (arrow) at the area of the fractured humerus. (d) Intraoperative photograph shows a distal radial nerve stump (arrow) 5 cm distal to the proximal stump. Figure 3b. Spiral fracture in an 18-year-old man (patient 3) who had complete motor and sensory paralysis. (a) Longitudinal US scan shows a hypoechoic enlarged radial nerve (solid arrows) with bulbous swelling at the disrupted proximal part (open arrow). (b) Longitudinal US scan shows a hypoechoic distal nerve stump (solid arrow) 5 cm distal to the proximal stump; the View larger version (121K): distal part of the nerve has a normal, [in this window] hyperechoic appearance (open arrow). (c) [in a new window] Intraoperative photograph shows a proximal amputation neuroma (arrow) at the area of the fractured humerus. (d) Intraoperative photograph shows a distal radial nerve stump (arrow) 5 cm distal to the proximal stump. Figure 3c. Spiral fracture in an 18-year-old man (patient 3) who had complete motor and sensory paralysis. (a) Longitudinal US scan shows a hypoechoic enlarged radial nerve (solid arrows) with bulbous swelling at the disrupted proximal part (open arrow). (b) Longitudinal US scan shows a hypoechoic distal nerve stump (solid arrow) 5 cm distal to the proximal stump; the View larger version (132K): distal part of the nerve has a normal, [in this window] hyperechoic appearance (open arrow). (c) [in a new window] Intraoperative photograph shows a proximal amputation neuroma (arrow) at the area of the fractured humerus. (d) Intraoperative photograph shows a distal radial nerve stump (arrow) 5 cm distal to the proximal stump. Figure 3d. Spiral fracture in an 18-year-old man (patient 3) who had complete motor and sensory paralysis. (a) Longitudinal US scan shows a hypoechoic enlarged radial nerve (solid arrows) with bulbous swelling at the disrupted proximal part (open arrow). (b) Longitudinal US scan shows a hypoechoic distal nerve stump (solid arrow) 5 cm distal to the proximal stump; the View larger version (147K): distal part of the nerve has a normal, [in this window] hyperechoic appearance (open arrow). (c) [in a new window] Intraoperative photograph shows a proximal amputation neuroma (arrow) at the area of the fractured humerus. (d) Intraoperative photograph shows a distal radial nerve stump (arrow) 5 cm distal to the proximal stump. Figure 4a. Comminuted fracture with a loose compression plate in a 72-year-old woman (patient 7), who had an incomplete motor deficit. (a) Longitudinal US scan shows the radial nerve riding on the proximal edge of the compression plate (open arrow). The nerve appears hypoechoic and enlarged (solid arrows) proximal to the injury. (b) Intraoperative View larger version (131K): photograph shows that the radial nerve appears [in this window] thickened at the proximal part (small arrows) [in a new window] and that there is a marginal defect (large arrow) corresponding to the nerve part that was riding on the plate. Figure 4b. Comminuted fracture with a loose compression plate in a 72-year-old woman (patient 7), who had an incomplete motor deficit. (a) Longitudinal US scan shows the radial nerve riding on the proximal edge of the compression plate (open arrow). The nerve appears hypoechoic and enlarged (solid arrows) proximal to the injury. (b) Intraoperative View larger version (139K): photograph shows that the radial nerve appears [in this window] [in a new window] thickened at the proximal part (small arrows) and that there is a marginal defect (large arrow) corresponding to the nerve part that was riding on the plate. The other six patients with humeral shaft fractures and radial nerve paralysis were treated conservatively with a thoracobrachial cast and percutaneous electrical nerve stimulation. US performed within 1–4 weeks after the trauma showed circumscribed swelling of the radial nerve, without evidence of laceration or entrapment at the area of the fracture. The echotexture of the nerve appeared abnormal, with loss of its normal fascicular pattern (Fig 5a). The mean anteroposterior diameter of the radial nerve in the fractured arm in these six patients was significantly larger (5.4 mm; range, 3.8–4.9 mm) than that of the noninjured arms and control group (2.5 mm; range, 2.2–3.0 mm) (P < .001); likewise, the mean mediolateral diameter was significantly larger (5.4 mm [range, 5.0–5.8 mm] versus 4.8 mm [range, 4.5–5.2 mm]) (P < .001). Figure 5a. Humeral fracture in a 38-year-old man (patient 4) who had primary complete motor radial palsy. (a) Longitudinal US scan shows continuity of the radial nerve with a circumscribed swelling (arrows), which suggests an intraaxonal lesion. (b) Follow-up longitudinal US scan, obtained 2 months after a, shows normalization of the radial nerve View larger version (132K): (arrows). [in this window] [in a new window] Figure 5b. Humeral fracture in a 38-year-old man (patient 4) who had primary complete motor radial palsy. (a) Longitudinal US scan shows continuity of the radial nerve with a circumscribed swelling (arrows), which suggests an intraaxonal lesion. (b) Follow-up longitudinal US scan, obtained 2 months after a, shows normalization of the radial nerve View larger version (128K): (arrows). [in this window] [in a new window] At 6-month follow-up in these six patients, two showed complete functional recovery, two had persistent slight motor and sensory deficits, and two had persistent sensory discomfort. US showed complete normalization of the size and echotexture of the radial nerve in all six cases. A representative US follow-up examination in a patient with conservative treatment and normalization of the nerve size after 6 weeks is demonstrated in Figure 5. TOP ABSTRACT INTRODUCTION MATERIALS AND METHODS RESULTS DISCUSSION REFERENCES DISCUSSION Investigators in previous studies (19–25) have reported the appearance of normal and abnormal peripheral nerves in compartment syndromes. In only one study (24), however, was the course and diameter of the normal radial nerve shown by using US. The size and anatomic characteristics of the normal radial nerve as described in that study corresponded well with our findings. In addition, we detected that the radial nerve changed its shape from round at the proximal third of the humerus to oval at the middle third and then to round again at the distal third of the humerus on the transverse scan. The oval shape of the nerve at the spiral groove may be explained by the close relationship of the nerve with the bone. Typically, the deep brachial artery was found adjacent to the radial nerve at the spiral groove; this finding can be well demonstrated with power Doppler US (Fig 2b). There is general agreement that radial nerve injury in cases of open humeral fracture, associated with vascular injuries or requiring bone débridement, needs early surgical repair (1,3,4,7,8). From a reconstructive point of view, an injured peripheral nerve has to be treated within 6 months to regain an optimal functional outcome; otherwise, irreversible muscle atrophy may occur due to degeneration of the motor end plate (9,11,27). Completely dissected or severely damaged nerves have the worst prognosis for regeneration (9,27). With regard to the criteria for conservative and surgical treatment in fractureassociated radial nerve palsy, which are controversially discussed in the literature (1– 11), obviously an imaging method that provides information regarding the integrity of the radial nerve is lacking. Even electroneurography and electromyography cannot be performed to distinguish between a damaged or disconnected nerve in the acute phase (27) and only permit monitoring of the reinnervation of a previously denervated muscle for 2–4 months after injury. Furthermore, the cause of the nerve impairment cannot be assessed from electrophysiologic testing, and no anatomic information can be obtained regarding the integrity of the nerve. This is especially seen when nerve regeneration is hampered by callous entrapment or scar tissue, or when the nerve is riding on the edge of a fracture fragment (3,4,14–16). In five of the 11 patients, US depicted severe nerve damage that required surgical repair and allowed specification of the nature of the nerve impediment. The intraoperative findings corresponded with those of presurgical US in all of these cases. The damaged radial nerve appeared hypoechoic and had loss of the normal fascicular pattern at the level of the humeral fracture. Similar findings of a swelling and hypoechoic echotexture from the nerve were described in several studies in which carpal tunnel and ulnar compression syndromes were evaluated (23,25). Although the results of electromyography and electroneurography indicated complete motor paralysis in eight of the 11 patients, US enabled detection of fascicular hematoma without severe nerve damage in four of these patients. These four patients received conservative therapy and recovered completely within 6 months. A limiting factor of US when interpreting abnormal peripheral nerve conditions is that it requires an experienced operator with a profound knowledge of the US appearance of different soft-tissue structures and requires US equipment of advanced technologic quality with high-frequency linear-array transducers. The detection of peripheral nerves with US, however, is reduced especially when the nerve lies deeper than 3 cm and a linear-array transducer of less than 7 MHz is used (20). US equipment with harmonic imaging capabilities or multidirectional scanning heads may help to increase spatial resolution and minimize technical errors; it may also widen the diagnostic perspective to other traumatic peripheral nerve injuries. In conclusion, our results show that US can be performed to demarcate the radial nerve in normal and posttraumatic conditions. US permits identification of the radial nerve in patients with humeral shaft fracture and associated nerve palsy. Our preliminary results suggest that severe damage to the radial nerve, such as laceration or gross impingement by displaced bone fragments, scar tissue, or callus, can be visualized with US. This information contributes to the decision as to whether surgical or conservative treatment is needed. US also provides the surgeon with important information concerning surgical exploration and reconstruction. Accurate visualization of the injured nerve can help to shorten the time gap between injury and treatment. Furthermore, US appears to be a helpful noninvasive tool for monitoring nerve regeneration and can be easily repeated at a low cost. Further prospective studies should be performed to assess the reliability of US in posttraumatic nerve paralysis. Upcoming technical developments will improve the spatial resolution and lead to a more accurate delineation of abnormal peripheral nerve conditions.