LOWER GI Suspected Cancer Referral
advertisement

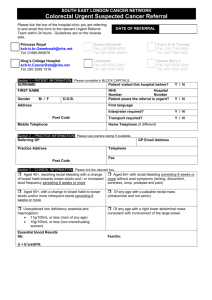
LOWER GI Suspected Cancer Referral (2 Week Wait Referral) To support NICE guidance 2005 Please FAX within 24 hours to Cancer Pathways department on: 020 8928 8836 Section 1 PATIENT INFORMATION (Please complete in BLOCK CAPITALS) Date of Referral Date of Birth NHS number UBRN SURNAME FIRST NAME Miss Mrs Ms Mr Other:_________ / / / / - - Home Tel. M[ ]F [ ] Mobile/Daytime Tel. Address Transport Y N Interpreter Y N Language Ethnicity Post Code Section 2 PRACTICE INFORMATION (Please use practice stamp if available) Referring GP Locum Practice Address Y N Telephone Fax Post Code Section 3 CLINICAL INFORMATION (please TICK all applicable entries) Please enclose print outs of CURRENT medications and PAST MEDICAL HISTORY All ages [ ] Definite, palpable, right sided, abdominal mass [ ] Definite, palpable, rectal (not pelvic) mass [ ] Unexplained iron deficiency anaemia AND: [ ] Male with a Hb of < 11g/dl [ ] Non menstruating female with a Hb of < 10g/dl Over 40 years [ ] Rectal bleeding WITH a change of bowel habit towards looser stools &/or increased frequency 6 wks Medical History, Known Allergies All Medication DIABETIC: YES/NO WARFARIN: YES/NO CLOPIDROGREL: YES/NO Over 60 years [ ] Rectal bleeding persisting 6wks WITHOUT a change in bowel habit or anal symptoms (e.g. soreness, discomfort, itching, prolapse, pain) [ ] Change in bowel habit to looser stools &/or more frequent stools persisting 6 wks WITHOUT rectal bleeding Mandatory Investigations [ ] PR examination [ ] Abdo examination Findings: [ ] FBC: Hb:____ MCV ___ Date: __ /__/__ Family History incl. relative and age at diagnosis Fitness Rating (ECOG) Please circle approp. no.: 0 Fully active 3 Able to carry out limited self-care, 1 Unable to do strenuous activities mainly confined to bed or chair 2 Able to walk and self-care 4 Completely confined to bed or chair Discussed urgent suspected cancer referral with patient: Y N Your patient may go straight to a diagnostic test, for example, Colonoscopy, Flexi sigmoidoscopy, CT abdo pelvis. In your opinion would this patient be suitable to go straight to a diagnostic test? Yes / No Have you told the patient they may go straight to a diagnostic test? Yes / No Comments/other reasons for urgent referral: Hospital use only: (Tick where appropriate) Date Appointment Booked: Target Dates 2ww 62/7 / / / / / / Date of Referral receipt: Database: / Patient confirmed: / A separate letter only need accompany if you feel it necessary To be Approved by the North East London Cancer Network April 2006 LOCAL CONTACT DETAILS If you wish to discuss any clinical issues concerning this referral please contact: Mr Michael Machesney Mr Pasquale Giordano Kitty Aristides Consultant Colorectal Surgeon Consultant Colorectal Surgeon Lower GI Nurse Specialist 020 8535 6066 020 8535 6656 0208 539 5522 -Bleep 676 If you wish to discuss any other aspect of this referral please contact the Cancer Pathways Office on 020 8535 6856/ 020 8535 6768 x4348 x4350 CRITERIA FOR URGENT SUSPECTED CANCER REFERRAL1 Please FAX the referral form within 24 hours Refer a patient who presents with symptoms suggestive of colorectal or anal cancer to a team specialising in the management of lower gastrointestinal cancer, depending on local arrangements. Investigations Always carry out a digital rectal examination in patients with unexplained symptoms related to the lower gastrointestinal tract. Where symptoms are equivocal a full blood count may help in identifying the possibility of colorectal cancer by demonstrating iron deficiency anaemia, which should then determine if a referral should be made and its urgency. When referring, a full blood count will assist specialist assessment in the outpatient clinic. When referring, no examinations or investigations other than abdominal and rectal examination and FBC are recommended as this may delay referral Risk factors Offer patients with ulcerative colitis or a history of ulcerative colitis a follow-up plan agreed with a specialist in an effort to detect colorectal cancer in this high-risk group. Low Risk Criteria Patients of all ages with the following symptoms and no abdominal or rectal mass are at very low risk of colorectal cancer and should therefore not be referred under the two-week system: Rectal bleeding WITH anal symptoms, e.g. soreness, discomfort, itching, lumps, prolapse and pain Rectal bleeding with an obvious external cause for bleeding on simple examination of the perineum, e.g. anal fissure, thrombosed or prolapsed pile and rectal prolapse Transient changes in bowel habit, particularly to harder stools and/or decreased frequency of defecation Abdominal pain as a single symptom WITHOUT other higher risk age/symptom/sign profiles, an abdominal mass, an iron deficiency anaemia or intestinal obstruction If your patient fits these “low risk” criteria, please do not use this form Refer the patient by means of a routine referral letter Fitness rating or ECOG The ECOG (Eastern Cooperative Oncology Group) performance score: 0 = fully active, the same as before suspicion of cancer 1 = unable to do strenuous activities but still able to do tasks such as light housework or office work 2 = able to walk and carry out self-care (e.g. eating, dressing), but not able to work 3 = only able to carry out limited self-care, mainly confined to bed or chair 4 = completely confined to bed or chair and not able to carry out self-care 1 Based on Referral Guidelines for Suspected Cancer (NICE, 2005) Notes in grey refer to the evidence grading used in the NICE guidelines, for more information see www.nice.org.uk/cg027NICEguideline) 2 In this guideline, unexplained is defined as ‘a symptom(s) and/or sign(s) that has not led to a diagnosis being made by the primary care professional after initial assessment of the history, examination and primary care investigations (if any)’. In the context of this recommendation, unexplained means a patient whose anaemia is considered on the basis of a history and examination in primary care not to be related to other sources of blood loss (for example, ingestion of NSAIDs) or blood dyscrasia.