Congenital and Hereditary Retinal and Optic Nerve Disease

1
Genetics of Posterior Segement Disease
Sherry J. Bass, OD, Jerome Sherman, OD, Jerry Rapp, PhD
I.
Orphan Diseases a.
Definition
II.
Retinitis Pigmentosa a.
Prevalence b.
Clinical characteristics c.
Symptoms d.
Types e.
Diagnostic testing i.
SD-OCT ii.
RNFL assessment: RNFL is above normal thickness except in later stages of the disease iii.
ERG iv.
Fundus Autofluorescence v.
Visual Fields f.
Hereditary patterns of RP g.
Differential from cone-rod dystrophies h.
Genetics i.
Dominant RP Genes
1.
RHO (Rhodopsin)-30%
2.
Peripherin/human Retinal degeneration Slow (RDS -10% ii.
Recessive iii.
X-linked RP
1.
RPGR gene (75%)
2.
RP2 (25%) i.
Treatment
III.
Leber Congenital Amaurosis a.
Prevalence b.
Clinical characteristics c.
Symptoms d.
Diagnostic tests i.
SD-OCT ii.
ERG. e.
Types f.
Hereditary patterns g.
Genetics h .
.
V a l l u e o f f m o l l e c u l l a r r g e n e t t i i c t t e s s t t i i n g i i n t t h e d i i a g n o s s i i s s o f f L C A i.
T r r e a t t m e n t t i.
H u m a n c l l i i n i i c a l l t t r r i i a l l s
IV.
ABCA-4 Dystrophies : ABCA4 =Transporter gene
1
2 a.
Stargardt Disease/ Fundus Flavimaculatus i.
Prevalence ii.
Clinical characteristics (may include one or more) iii.
Symptoms iv.
Diagnostic testing
1.
ERG
2.
FA
3.
VF
4.
Fundus autofluorescence imaging: v.
Hereditary patterns
1.
AR
2.
AD: Stargardt-Like Dystrophy (ELOVL mutations) vi.
Differential Diagnosis from other White Dot Diseases vii.
Genetics
1.
Known ABCA-4 mutations on short arm of chromosome 1 account for 50% of cases b.
Other ABCA-4 Dystrophies i.
Cone and Cone-rod dystrophy ii.
AMD (1-2%)
V.
Age-Related Macular Degeneration
A.
The Dawn of Pharmaco-Genetics in AMD a.
Rationale for Pharmacogenetics i.
AMD is the most common etiology of vision loss in the US.
The AREDS 1 and 2 studies confirm that anti-oxidants and zinc can reduce the risk of progressing from Category 3 AMD to more serious vision loss by about 25%. ii.
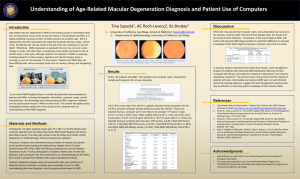
Based upon a landmark study published in Aug 2013 in the journal Ophthalmology, the presence or absence of high risk alleles in CFH and ARMS2 genes determines the most effective nutraceutical for each patient. b.
Introduction i.
What is AMD and how common is AMD? ii.
Age related? Race related? c.
Genetic and environmental considerations d.
Diagnostic Modalities i.
Standard Fundus Exam ii.
SD OCT iii.
Fluorescein angiography (FA) iv.
Fundus Autofluorescence (FAF)
2
3 v.
Preferential hyperacuity perimetry (PHP) and Home PHP e.
Genetics of AMD i.
12 known genes define nearly all of AMD genetic risk ii.
Genetics can now predict the 2,5, and 10 year risk of marked vision loss iii.
Genetic risk can be stratified into one of five categories
1.
Determines type and frequency of follow-up
2.
Best estimate: Genetic and epigenetic considerations a.
Smoking history plays a role b.
Systemic diseases play a role
3.
Significance of peripheral drusen f.
Nutritional considerations i.
Carotenoids ii.
Omega 3’s g.
AREDS 1 Results and Implications h.
AREDS 2 Results and Implications i.
What are the appropriate nutraceuticals for each patient?
B.
Treatment of Wet AMD a.
Numerous studies support that intravitreal anti-VEGF injections are effective in preventing progression and can even improve vision if used in a timely fashion b.
Treatments are being investigated that will lengthen the time between treatments c.
Greographic atrophy does not respond to anti-VEGF treatment
C.
The Evolving Standard of Care in AMD a.
ODs are recently getting sued for poor detection of wet and dry AMD b.
Consider risk factors to provide better care as we have been doing in glaucoma for years
D.
Treatment of Stage 3 Intermediate AMD i.
Careful follow-up ii.
Consider changing anti-VEGF
1.
E.g. if Lucentis or Avastin are not working, Eyelea
E.
Future Considerations should be tried.
VI.
Other Macular Disorders a.
Pattern Dystrophies of the RPE i.
Clinical characteristics ii.
Symptoms iii.
Types iv.
Hereditary pattern
3
4 v.
Diagnostic Testing
1.
FA:
2.
SD-OCT: vi.
Genetics
1.
The peripherin/RDS gene in Butterfly-shaped pigment dystrophy b.
X-Linked Juvenile Retinoschisis i.
Clinical Characteristics ii.
Hereditary pattern iii.
Diagnostic testing
1.
SD-OCT:
2.
ERG: iv.
Treatment
1.
Dorzolamide 2% TID for 3-5 months may reduce foveal thickness and can improve VA v.
Genetics
1.
RS1 gene mutations-affect the retinoschisin protein that provides the retinal “glue” to keep the inner retinal layers together c.
Best’s Vitelliform Dystrophy i.
Clinical characteristics ii.
Diagnostic testing
1.
SD-OCT:
2.
EOG: iii.
Hereditary pattern-AD iv.
Differential from other lipofuscin vitelliform maculopathies v.
Genetics d.
Importance of Genetic Testing in Diagnosing Hereditary Retinal Disease i.
Pedigree construction ii.
Genetic testing e.
Finding a Clinical Trial to Investigate On-Going Research
VII.
The Role of the Optometrist as Genetic Counselor a.
Knowledge b.
Information c.
Risk Assessment d.
Support
4