Tran, Jennifer
advertisement

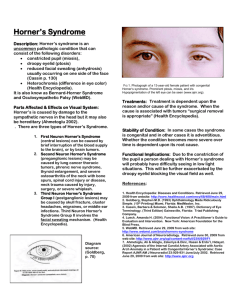
Acquired Horner’s Syndrome Jennifer Tran, O.D. Reno VAMC Resident Abstract: Etiologies of associated with Acquired Horner’s syndrome are stroke, pancoast syndrome, cluster headache and many more. The following case highlights the importance of pharmacologic test and imaging as part of diagnostic workup for Horner’s Syndrome. Case History: A 63 year-old male presented to the optometry clinic, needing new spectacles. His medical history was positive for hypertension and hyperlipidemia (both controlled on medications), headache syndrome of migraine and cluster type, and acquired Horner’s syndrome with symptoms of miosis, mild ptosis, and anhydrosis, which was diagnosed in 2004 by an outside medical provider. His migraine headaches were controlled with sumatriptan but provided no relief for cluster headache. His best corrected visual acuity was 20/20 OU. Patient was given a spectacle Rx and redirected to NeuroOphthalmology clinic for Horner’s syndrome follow up and dilated eye exam in one week. In the Neuro-ophthalmology clinic, patient revealed a positive history of automobile accident in 2004 that resulted in a left neck injury as well as the onset of his migraine and cluster headaches. Patient reported left ptosis that worsens with his cluster headaches episodes and they occur more often than his common migraines. His presentation of left Horner’s syndrome began with severe headache and nausea/vomiting about 5 years ago that was associated with nasal drainage and lacrimation with redness in his left eye. The patient reported anhydrosis in his left forehead concurrently with these cluster headaches. Pertinent findings: OS small 2mm, no reaction to light. OS miosis, mild ptosis ~2mm and absent heterochromia. Intraocular pressures were normal (12 mmHg OU). Otherwise unremarkable OU. The anisocoria is more prominent in dark illumination. Differential diagnosis: 1. 2. 3. 4. 5. Acquired Horner’s Syndrome associates with Cluster Headache Acquired Horner’s Syndrome associates with Trauma Acquired Horner’s Syndrome associates with stroke Acquired Horner’s Syndrome associates with carotid artery dissection Acquired Horner’s Syndrome associates with Pancoast Tumor Diagnosis and discussion: Acquired Horner’s Syndrome is a paralysis of sympathetic nerve supply causing miosis, ptosis, and anhydrosis but not heterochromia. The anisocoria is more pronounced in dim illumination where the Horner’s pupil is the smaller pupil. 10% cocaine test to determine for whether anisocornia is physiologic or caused by Horner’s syndrome, for horner’s of physiologic where the dilation lag of smaller pupil is present. 0.5% apraclonidine test is suggested if 10% cocaine is not available; in this test, the miotic eye with oculosympathetic defect dilates and the anisocoria reverses. The location of the sympathetic lesion can also be tested by using 1% Hydroxyamphatemine. Preganglionic or central lesions cause the pupils dilate normally, where the dilation does not occur in postgangionic third order neuron lesions. The oculosympathetic pathway has three neurons that lead to the sweat glands of the forehead, muller’s muscle, and the long ciliary nerves to the dilator pupillae. The first order neuron runs from the hypothalamus to the spinal cord. Stroke and multiple sclerosis most commonly affect the first order neuron. The second order neuron is on the spinal cord, thoracic cavity and lower neck, where Pancoast tumor or neck trauma can easily damage the nerve. The third order neuron is from the upper neck to the carotid arterial pathway. Carotid arterial dissection, cluster headache, and inflammation can damage the third order neuron based on its location. Many life-threaten etiologies are associated with new-onset Horner’s syndrome, and therefore the appropriate and timely pharmacologic test and imaging work-ups are necessary to rule out these serious causes. Cluster headache is a one-sided head pain around the eye, described as pressure against the eye. The pain usually lasts from 10 minutes to 2 hours and is more common in men than women (5:1 ratio). Lacrimation, redness and postnasal drip are common symptoms associated with cluster headaches. Partial Horner’s Syndrome occurs in 2 out of 3 of patients when they are examined during attacks. Cluster headache is highly associated with internal carotid dissection that can be fatal. One cause for cluster headache can be head trauma. The triggers for cluster headache include smoking, alcohol, bright light, or certain food. It’s important to educate patients with cluster and migraine headaches on smoking/alcohol cessation. Some treatment options for cluster headache include Lithium, Ca2+ channel blocker, and antihistamine. The treatment of cluster headache is aimed at pain relief. Imaging records in 2004 from outside medical provider revealed normal – no positive cause of Horner’s syndrome or cluster headaches. Pharmacologic tests with 10% cocaine and 1% hydroxyamphetamine were conducted in 2004 but poorly documented. Specific lesion location was not well documented. Given the classic history in this particular case, cluster headache causing a 3rd order neuron Horner’s syndrome is strongly suspected. Treatment, management: Timely and appropriate imaging work ups for a new onset Horner’s syndrome is MRI to rule out any stroke or Multiple sclerosis MRA/Carotid Ultrasound to rule out carotid artery dissection. Chest X-ray/CT to rule out Pancoast tumor Complete Blood Count to rule out any inflammation This patient declined Lithium as the recommended treatment for his cluster headaches. The patient is currently satisfied with his treatment regimen of Sumatriptan, which he uses approximately twice per month for his migraines. He prefers not to take additional medications for cluster headache prophylaxis since they are not that debilitating for him. Final diagnosis: Stable Acquired Horner’s Syndrome secondary to cluster headaches. Monitor annually with Neuroophthalmology prn for ocular problems or changes. Refer to research where appropriate: A Horner-like syndrome and cluster headache. What comes first? 1st Theory: ” Havalius H. A Horner-like syndrome and cluster headache, what comes first? Acta Ophthalmol Scand 2001; 79; 274-5” The finding indicate that a sympathetic lesion or dysfunction may be prerequisite for the subsequent development of cluster headache 2nd Theory: “Salvesen R. Cluster headache: are we only seeing the tip of the iceberg? Cephalalgia 1987;7:77–81” The first-order hypothalamic neuron generating ipsilateral symptoms papillary responsiveness and anhydrosis similar to Horner’s syndrome. 3rd Theory: “Gupta VK. Painless Horner’s syndrome in cluster headache. J. Neurol. Neurosurg. Psychiatry 1996; 60; 462463” Pain around and above the eye can be produced by stretching the internal carotid artery just below the syphon. Current literature still has no definite answer on which come first. It’s important to recognize the new onset symptoms and know what to do. The case highlights the importance of extensive imaging work up for acquired Horner’s syndrome and cluster headache symptoms to rule out more life-threaten etiology. References: 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. F. Hampton Roy, Ocular differential diagnosis, 5th ed 1993 page 70-72 M. Friedberg et all, The wills eye manual, 5th ed, 2008 pg 228-229 http://www.nlm.nih.gov/medlineplus/ency/article/000786.htm Murphy MA . Recurrent isolated horner syndrome. J Neuroophthalmol. 26(4); 196, 2006 Dec. Havalius H. A Horner-like syndrome and cluster headache, what comes first? Acta Ophthalmol Scand 2001; 79; 274-5 Salvesen R. Cluster headchae since headache; case report. Neurology 2001; 55; 451 Gupta VK. Painless Horner’s syndrome in cluster headache. J. Neurol. Neurosurg. Psychiatry 1996; 60; 462-463 Peatfield RC. Recurrence of cluster headaches presenting with virtually painless Horner’s Syndrome. J Neurol Neurosurg Psychiatry. 1995 August; 59(2): 196–197 http://www.clusterheadaches.com/about.html Data from Manzoni, G. C., Terzano; M. G., Bono, G. et al (1983b): Cluster headache - clinical findings in 180 patients. Cephalalgia 3:21-30 Giuseppe et all , Pupil responsiveness in cluster headache: A dynamic TV pupillometric evaluation. Cephalalgia 1998 8(3);193-201. Salvesen R. Cluster headache: are we only seeing the tip of the iceberg? Cephalalgia 1987;7:77–81 Clinical pearls: The presentation of Horner’s Syndrome - miosis, ptosis, anhydrosis, without heterochromia (congenital most commonly) Painful Acquire Horner’s Syndrome requires emergent medical work-up Acquired Horner’s Syndrome associates with cluster headaches. Timely and appropriate pharmacologic test and imaging work up for Acquire Horner’s Syndrome MRI, MRA, carotid ultrasound, Chest X-ray/CT, and Complete blood count.