British Orthopaedic Association PROCEDURE: Your forearm bones
advertisement

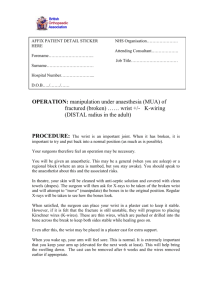
British Orthopaedic Association AFFIX PATIENT DETAIL STICKER HERE NHS Organisation…………………. Attending Consultant………………. Forename………………………….. Job Title…………………………… Surname…………………………… Hospital Number…………………... D.O.B…../……./…… OPERATION: MUA and ORIF of ………… RADIUS & ULNA (plate and screws to fix both forearm bones) - 2 incisions PROCEDURE: Your forearm bones (called the radius and ulna) are broken. Your surgeon feels that they will heal best if both fixed and held in position by plate and screws. Usually you will be put to sleep (general anaesthetic) although sometimes, the anaesthetic doctor may perform a regional block (when an area is numbed but you remain awake). You must discuss this with your anaesthetist. When in theatre, you will lay on your back with your arm outstretched. There are two bones broken and most surgeons make two cuts (incisions) to get to the bones. One will be on the front of the forearm and the other on the back. The size and exact position depend on you breaks. The surgeon must move muscle, tendons and delicately move blood vessels and nerves out of the way to get to the bone. Once there, your surgeon will position the ends in as close to normal position is possible and hold them with a plate and screws. When happy, the surgeon will start to close up the arm. Special skin stitches are used (sutures) these may dissolvable under the skin or above the skin. Those left above the skin will need to be removed at 10 to 14 days. Check with your surgeon. Often the surgeon likes to keep the arm in a plaster for added protection. The time in a plaster depends upon the type of break and the surgeon. British Orthopaedic Association You will be encouraged to keep your arm held high (elevated) after the operation - this is important as it keeps the swelling down. ***Please be aware a surgeon other than the consultant, but with adequate training or supervision may perform the operation*** ALTERNATIVE PROCEDURE: the fracture may be left in its current position in a plaster. If it is not in a good solid position, it may not heal as well or the function of your elbow or wrist may be affected. This will make it more likely refracturing (rebreaking), arthritis, pain and disability. You may of course seek a second opinion. There may be other forms of fixation, such as wiring or external fixators. These may not be appropriate for your case. You should discuss these with your consultant. RISKS As with all procedures, this carries some risks and complications. COMMON (1-5%) Pain: your wrist will be sore after the operation. Keeping the arm up (elevated) most of the time will help reduce the pain and swelling. We will also give you pain killers. If you need more, however, please ask a member of staff. Bleeding: There will almost certainly be some bleeding. This is usually small spotting and will stop itself. Very rarely, a blood vessel is damaged and there is more bleeding or it may form a clot. This may need a second operation to stop the bleeding or remove the clot. RARE (<1%) Infection: unfortunately, even though the surgeon inserts the plate in theatre where everything is sterile and your skin is cleaned, there is still a small percent of patients who develop an infection. Most infections will present as redness, swelling or even a discharge of fluid or pus. A course of antibiotic may be needed. If the infection is severe, a further operation including removal of plate may be necessary. Neurovascular damage: there are numerous blood vessels and nerves that run through and around the wrist. This means that they may be damaged by the plate as it is put in. This might lead to numbness or weakness of muscles. This may be temporary or in very rare cases, permanent. Compartment syndrome: this is a build up pressure within the forearm and can cause pain, nerve damage, blood vessel damage and muscle damage. If this occurs, an emergency operation will have to be performed. British Orthopaedic Association Slipped position; Despite manipulation, plating and cast application, the fracture may very rarely still slip. Further operation may be necessary. Removal of metalwork: This is not usually necessary in adults unless there is pain, infection or severe restriction in movement or irritating the skin. In children who are still growing, the plate is usually removed. This is often around 12 weeks after the break. Arthritis- and stiffness at the wrist or elbow may occur despite adequate reduction. Arthritis may be more common if the fracture involves the joint. CRP syndrome: this is pain, swelling or stiffness around the fracture site and may occur even months after the original injury. Rebreak: the bones can Rebreak and Confirmation of consent : The doctor has explained the above complications, risks and alternative treatments to me as well as not having the procedure. I hereby give my consent for the above procedure Signature…………………………………………………. Print name……………………………………………………….... Date………./…/20… 2nd Confirmation………………...............…… .Date…………./…..20…. NAME of SURGEON (Capital letters)……………………………….. NAME of SURGEON (Capital letters)……………………………….. SIGNATURE of SURGEON…………………………………………. SIGNATURE of SURGEON…………………………………………. POSITION…………………………………………………………….. POSITION…………………………………………………………….. If you have any complaints about your treatment or your care, you are always encouraged to discuss them with your surgical team. However, if you wish to complain to the trust, each hospital will have a PALS or Patient Advise and Liaison Service. The head nurse on the ward or out patients’ clinic can direct you to them. The PALS team will treat all complaints seriously. I also give consent for my notes any data recorded to be used in any current or future research Signature…………………………………………Date……………………..