Arterial Blood Gas Sampling (ABG)
advertisement
")
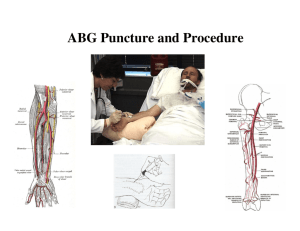
Arterial Blood Gas Sampling (ABG) Egan Chapter 18 I. Introduction – A. What are “blood gases”? a. They are gases (2) found in the blood a) O2 for cell metabolism and b) CO2 which is a by-product of that metabolism B. Why “arterial” blood gas sampling and not venous blood gas sampling? a. All arteries carry blood from a single anatomical part of the body, the cardiopulmonary system, this is oxygenated blood that has not been used up by the body a) veins carry blood from various different anatomical body parts (i.e.: hand, arm, leg) with varying metabolic rates. Veins pick up CO2 from tissue and carry it back to the lung to be expelled from the body. C. What is purpose of ABG’s? a. Diagnostic aid – b/c they reflect the efficiency of the CP system. a) Assess gas exchange b) Can diagnose respiratory failure (↑ CO2 with a ↓ pH) b. Indicator of the effectiveness of therapy. a) Does the oxygen gas flow have to be turned up, or can it be turned down (PaO2)? b) Is the patient ventilating effectively (PaCO2) and needs the mandatory respiratory rate adjusted when on mechanical ventilation D. How is the blood obtained? a. Arterial Puncture – from peripheral arteries (See Figure 18-2) B. Indwelling Catheter (arterial, central line, or PA line) C. Capillary Gas – finger or heel prick II. Arterial Puncture A. Blood is drawn through a needle puncture fro a peripheral artery. a. radial artery is preferred due to collateral circulation b. it is near the surface and easy to palpate c. not near any large veins d. relatively pain free (????) 1. other sites are riskier and only performed by personnel trained to draw fro the other sites. 2. arterial draws on infants take additional training 3. READ AARC GUIDELINES P. 369 4. READ BOX 18-3 CLINICAL INDICATIONS FOR ABG B. Preparation and Pre-analytical Considerations A. Patient status and infection control – a. Review the chart a) Doctors Order b) Primary Diagnosis c) Respiratory Care Modalities? 1. O2 therapy – ck for steady state 2. ventilator settings – wait 20-30’ post ventilator changes d) Anticoagulant Therapy? - reduces the bloods ability to clot and can ^ the risk of ^ bleeding following puncture. Use increased compression time. 1. Sodium Heparin (I.V.) 2. Warfarin Sodium compounds (Oral) 1) Coumadin 2) Prothomadin 3. Dipyridamole (Oral or I.V.) 4. excessive Aspirin ingestion 5. FOR USE in ABG SYRINE ONLY 1) Lithium Heparin or dry heparin 2) Sodium Heparin or wet heparin e) Thrombolytics – dissolves clots and can ^ the risk of bleeding following puncture. May need to use more compression time. 1. Streptokinase f) Bleeding Disorders? 1. Hemophilia – confirm with Dr. if ABG should be performed. (Can it be drawn fro a line or a heel stick?) 2. low platelet count (lab rpt) - ^ compression time 3. prolonged bleeding time – ^ compression time (lab rpt) 1) PT – Prothrombin Time Normal is 12 - 14 seconds ** Coumadin trx monitor (oral) 2) PTT - Partial Prothrombin Time Normal 38 - 42 seconds ** heparin trx monitor (I.V.) f) Infection Control – Trx all blood as infected. Always wear gloves, do not contaminate inanimate objects, wear mask and goggles, wash hands and observe other standard precautions. Guard against accidental needle sticks. 1. HIV 2. viral hepatitis 3. syphilis (CONTINUED…..) 4. Jacob-Creutzfeldt disease 1) rare fatal encephalopathy 5. septicemia B. “Steady State” – p. 372 - blood gases are dynamic and a period of continuous therapy (FIO2 and CMV settings) must elapse so that gases in the blood reach an equilibrium. a. Normal patient with no chronic condition a) 5 - 10 minutes b. Pt with COPD a) 20 - 30 minutes C. Document current status - VERY IMPORTANT for data to be useful a. FIO2 (or device w flow) x # minutes b. CMV settings x # minutes c. puncture site (RB, LB, RR, LR) d. time and date sample drawn e. pt. position (V/Q assessment) D. Materials – See kit contents READ BOX 18-1 ON PAGE 368 E. Local Anesthetic – NOT OFTEN USED sometimes used in pediatrics and small children to allow pt. to calm down, equilibrate and thus get an accurate sample a. 0.5% lidocaine (1/4 cc) is injected under the skin and around the puncture site via a 25G tuberculin syringe III. Complications of Arterial Puncture (4 plus)– A. Thrombosis - the formation of a clot within a vessel (thrombus) a. blockage of a vessel can result in necrosis of distal tissue a) loss of the thumb and index finger perform the Allen Test (See handout) b) loss of a foot or lower leg B. Hematoma (blood tumor [swelling]) – results from the leakage of blood into the surrounding tissue. a. can be large and compress the artery C. Arteriospasm – due to pain or anxiety a. can cause blockage of the artery b. time or a warm compress can relax the spasm D. Other a. extreme pain b. infection c. peripheral nerve damage d. Vasovagal (vascular & vagal) response 1) precordial distress – discomfort over the heart & 2) 3) 4) 5) stomach anxiety feeling of impending doom nausea respiratory difficulty IV. Anatomical Landmarks for Puncture Site & Local Nerve A. Radial Puncture Site a. above the crease of the wrist: 1 - 2 cm or 0.4 - 0.8 inches (about a half of an inch) b. extend wrist to about 30° c. 450 angle or steeper - needle to surface of the skin. d. depth is just below the surface of the skin to 0.5 inch (obesity) e. Radial Nerve is lateral to the puncture site and generally. behind the radial bone. B. Brachial Puncture Site a. above the crease of the elbow. Just above. b. medial in relation to the anterior elbow (normal anatomical position) 0 c. 60 degree angle or steeper - needle to the surface of the skin. d. depth is just below the surface of the skin (cachexia) to 0.8 inch (obesity) e. Medial Nerve is lateral and VERY close to the puncture site C. Femoral Puncture Site a. below the fold of the groin. 0.25 to 0.5 inch (must miss the inguinal ligament) b. middle of the superior side of the femoral triangle c. 900 angle - needle to the surface of the skin d. depth is 0.5 (cachexia) to 2.0 inches or more (obesity) e. Femoral Nerve is lateral and against the femoral artery f. Femoral Vein is medial and against the femoral artery V. Arterial Puncture Technique – READ BOX 18-2 ON PAGE 370 A. STUDY "ABG Sampling Laboratory Performance" for proper techniques for three puncture sites B. ALWAYS – * Do modified Allens test (SEE Figure 18-3) * Get comfortable (sit in a chair, lower bedrails) and do not rush. * Hold syringe with dominant hand * Place gauze near non dominant hand. * Place needle stopper near dominant hand. Avoids accidents. * NEVER LOOSEN GRIP on syringe (control your breathing and avoid any movements once blood begins to flow) as the arterial puncture will be lost and hematoma can result. * As syringe fills with blood, place gauze over needle entry point and wait for barrel to fill. * Place FAIR pressure upon puncture site and quickly withdraw needle. * Place FIRM pressure (above systolic mm Hg) on puncture site. * HOLD PRESSURE for a minimum of FIVE MINUTES (watch time). * Most hospital policies allow for only TWO advances of the needle after which another RCP must be called C. Allen Test – a test for collateral circulation around the Radial puncture site (via the Ulnar and Palmer Arch arteries) * There is NO collateral circulation around the Brachial or Femoral Artery puncture sites. VI. Procedure for Drawing Gases from Indwelling Catheters READ BOX 18-4 ON PAGE 374 VII. PROCEDURE FOR CAP GAS SAMPLING READ BOX 18-5 ON PAGE 376 AARC GUIDELINES P. 375 VIII. Advantages and Disadvantages for each Puncture Site A. Radial Puncture Site a. closest to the surface of the skin b. little chance of nerve trauma c. no esthetic objections (also spelled aesthetic taste or conscious of something) d. easy to detect hematoma e. easy to compress - one finger f. smallest of 3 puncture sites g. can test for collateral circulation B. Brachial Puncture Site a. not as deep as femoral site b. much greater (than radial) chance of nerve trauma c. no esthetic objections (vs. femoral site) d. more difficult (than radial) to detect hematoma e. harder than radial to compress - 2 or three fingers f. larger than radial vessel g. can NOT test for collateral circulation C. Femoral Puncture Site a. deepest of all three puncture sites b. greatest chance of nerve trauma c. esthetic objections do exist d. can NOT detect hematoma e. hardest to compress - hand over 4 fingers or palm f. largest of all three vessels g. can NOT test for collateral circulation IX. Troubleshooting and Problem Solving A. Getting a Good Sample a. READ p. 371 b. Always withdraw needle before redirecting in case you have gone through the artery. c. If the needle is completely withdrawn you must open a new ABG kit. d. If you must apply suction it is probably a venous sample unless it is smaller than a 23 gauge needle. Due to the size of these small needles you may have a apply a very small amount of pull on the syringe barrel. B. Pre Analytical Errors Table 18-1 p. 371 a. Most Preanalytical errors can be avoided by: *obtaining sample anaerobically (without air) *it is properly anticoagulated * any air bubbles are immediately expelled * analyzed within 15 minutes C. Read paragraph on blood cell metabolism on p. 371 (chill or not to chill) X. PROCEDURE FOR ANALYZING A BLOOD GAS SAMPLE READ BOX 18-6 ON PAGE 378 -END-