Refeeding Syndrome
advertisement

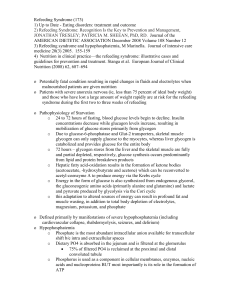
Refeeding Syndrome Bruno Schneeweiss, M.D. and Christian Zauner*, M.D. Dept. of Internal Medicine, Landeskrankenhaus Kirchdorf/Krems, Austria phone +43-7582-696-3581, fax +43-7582-696-3504, e-mail: bruno.schneeweisz@univie.ac.at and *Dept. of Internal Medicine IV, University of Vienna, Austria Learning Objectives To identify patients at risk for refeeding syndrome To list the mechanisms involved in the pathogenesis of refeeding syndrome To list measures to be taken for the prevention or treatment of refeeding syndrome Definition Refeeding syndrome is defined as a derangements in serum electrolytes (phosphate, potassium, magnesium), vitamin deficiency, and fluid as well as sodium retention occurring in malnourished patients after initiation of parenteral nutrition [1,2]. The limitation of the term “refeeding syndrome” only to patients receiving parenteral nutrition is not justified, since these changes in metabolism have also been found in orally fed patients after long-term starvation [3,4]. Pathogenesis of Hypophosphatemia In starvation and other catabolic illness loss of fat and lean body mass is accompanied by a proportional loss of phosphate, although the blood phosphate concentration is still kept in the normal range. In starvation the energy needs are provided mainly by the oxidation of fat. For beta-oxidation of fatty acids to be operative the phosphorylation of substrates is not necessary. On refeeding with glucose-based nutritional regimens, however, inorganic phosphate is needed for phosphorylation of glucose which in this form enters glycolysis. During glucose supply endogenous insulin secretion is stimulated or insulin must be administered exogenously to maintain normoglycemia. Hyperinsulinism leads to protein synthesis accompanied by a transfer of glucose and phosphate into cells. The combined effects of phosphate loss during starvation and increased insulin-mediated transport of phosphate from the extracellular to the intracellular compartment during refeeding with glucose can lead to a dramatic drop in blood phosphate concentration [5,6]. Consequences of Hypophosphatemia during Refeeding Phosphate is essential for many metabolic processes. It is crucial for a normal function of erythrocytes, leucocytes, platelets, for oxygen liberation from oxy-hemoglobin, for ATP synthesis, and normal function of the central nervous system [6]. Since phosphate is mainly found in the intracellular compartment, serum concentrations do not reflect intracellular concentration accurately. Furthermore, serum phosphate concentrations show a diurnal variation. Therefore, the clinical consequences of hypophosphatemia cannot be predicted by the actual serum concentration of phosphate. Severe hypophosphatemia is defined as a serum phosphate concentration below 0.32 mmol/L and can cause severe neuro-muscular and cardiovascular dysfunction. Lifethreatening cardiopulmonary and neurological complications have been observed on the refeeding of severely malnourished patients during the second world war and in patients receiving a phosphate-free hyperalimentation containing glucose [7]. However, severe hypophosphatemia accompanied with life-threatening dysfunction has also been reported in patients after the institution of enteral nutrition [8]. Even in moderate hypophosphatemia (serum phosphate concentrations between 0.32 – 0.35 mmol/L) reduced diaphragmal contractility, ventricular arrhythmia, reduced cardiac function, and insulin resistance have been found. Marik and Bedigian diagnosed hypophosphatemia induced by refeeding in 34% of critically ill patients after initiation of feeding even with a phosphate-supplemented nutritional regimen. The only risk factor predicting hypophosphatemia was a serum pre-albumin concentration of <110g/L (serum pre-albumin concentration is a good marker of malnutrition in hospitalised patients). Body weight was also decreased in patients who developed hypophosphatemia. However, this difference did not reach statistical significance. The severity of illness expressed by the APACHE II score was not different between patients with or without hypophosphatemia. The length of hospital stay and the duration of ventilator dependency was increased in patients with hypophosphatemia. Treatment of Hypophosphatemia It is essential to prevent refeeding-induced hypophosphatemia by recognising patients at risk (e.g. malnourished patients with anorexia nervosa, chronic malabsorption syndromes, chronic alcoholism, or patients with massive weight loss). During refeeding energy supply should be initiated slowly and serum concentrations of electrolytes should be closely monitored. After the development of hypophosphatemia phosphate has to be supplied in an appropriate amount: Moderate to severe hypophosphatemia: phosphate supply of 0.02 – 0.03 mmol/kg/h to reach a serum concentration of 0.65 mmol/L [9]. Rosen et al. found that even a higher rate of administration (15 mmol phosphate within two hours) is safe and sufficient in correcting hypophosphatemia in critically ill patients [10]. Hypokalemia and Hypomagnesemia These disturbances in electrolyte metabolism have also been described in malnourished patients and can also be accompanied by neuro-muscular dysfunction and cardiac arrhythmia. Although Marik and Bedigian found hypophosphatemia in 34% of their critically ill patients after initiation of nutritional support, they could not detect any derangements of the potassium and magnesium levels [6]. Serum concentrations of these electrolytes should also be monitored closely during the initiation of refeeding. If hypokalemia or hypomagnesemia develop, these electrolytes should be supplied accordingly. Hyperammonemia During prolonged starvation a reduction in protein degradation in muscle and other tissues is the consequence of adaptive metabolic mechanisms. The activity of enzymes of aminoacid metabolism is reduced, which can lead to an increased plasma concentration of amino acids during refeeding. The concentration of amino acids in blood can exceed the capacity of the urea cycle and thus, hyperammonemia may occur. The death of patients with severe malnutrition refed with a protein-rich diet has been attributed to this metabolic derangement [4]. Hyperammonemia can be prevented by increasing energy supply slowly during refeeding. Diarrhea Diarrhea is often found in starving and malnourished patients and can be exaggerated by oral refeeding. Enterocyte dysfunction and atrophy of the intestinal mucosa can originate from starvation and result in a reduction in absorptive capacity to the extent that malabsorption and osmotic diarrhea may occur during refeeding. Also, an increased mucosal secretion has also been discussed as a cause of diarrhea [11]. References 1. Solomon SM, Kirby DF. The refeeding syndrome. A review. J Parent Enteral Nutr 1990; 14: 90-97 2. Brooks MJ, Melnik G. The refeeding syndrome: an approach to understanding its complications and preventing its occurrence. Pharmacotherapy 1995; 15: 713-26 3. Schnitker MA. A clinical study of malnutrition in Japanese prisoners of war. Ann Int Med 1951; 35: 69-96 4. Freeland RA, Briggs S. A biochemical approach to nutrition. London: Chapman & Hall, 1977 5. Knochel JP. The pathophysiology and clinical characteristics of severe hypophosphatemia. Ann Int Med 1977; 137: 203-220 6. Marik PE, Bedigian MK. Refeeding hypophosphatemia in critically ill patients in an intensive care unit. A prospective study. Arch Surg 1996; 131: 1043-1047 7. Sivis SE, Paragas PD. Paresthesias, weakness, seizures and hypophosphatemia in patients receiving hyperalimentation. Gastroenterology 1972; 62: 513-520 8. Hayek ME, Eisenberg PG. Severe hypophosphatemia following the institution of enteral feedings. Arch Surg 1989; 124: 1325-1328 9. Havala T, Shronts E. Managing the complications associated with refeeding. Nutr Clin Pract 1990; 5: 23-29 10. Rosen GH, Boullata JI, O'Rangers EA, Enow NB, Shin B. Intravenous phosphate repletion regimen for critically ill patients with moderate hypophosphatemia. Crit Care Med 1995; 23: 1204-1210 11. Hedwig-Larson P. Famine disease in German concentration camps: compensations and sequels. Acta Med Scand 1952; 274(suppl.): 1-60