Anesthesia Pain Management Service
advertisement

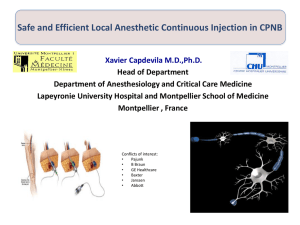
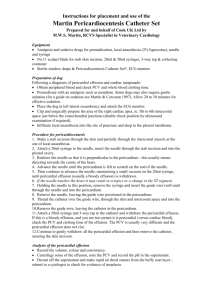
Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 If a patient is a candidate for regional anesthesia: Consider potential contraindications 1. Presence of an active infection at the site of puncture 2. True allergy to amide local anesthetics 3. Anticoagulation: follow guidelines for neuraxial techniques for deep lumbar plexus blocks and paravertebral blocks Regional Block/Catheter Types and Indications: Interscalene block: surgery on shoulder, distal clavicle and proximal humerus Supraclavicular block: surgery on humerus, elbow and hand Infraclavicular block: surgery on humerus, elbow and hand (rarely performed at MMC/SSC) Axillary block: surgery on elbow, forearm and hand (rarely performed at MMC/SSC) Femoral nerve block for total knee arthroplasty Femoral catheter: surgery on femur, anterior thigh and knee. Femoral nerve catheter/SNB (popiteal or gluteal) for above knee amputation (AKA). FN=Femoral Nerve FA=Femoral Artery JVP/PM/OWN/MB 2014 Spectrum Medical Group So. Anesthesiology Division Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 Sciatic catheter: for surgery at and below the knee. Sciatic catheter/FNB for below knee amputation (BKA). Posterior approach to ultrasound-guided popliteal sciatic block can be performed with the patient in the oblique position or with the patient prone Sonoanatomy of the popliteal fossa with the structures labeled. TN(Tibial Nerve) and CPN(Common Popliteal Nerve) are lateral and superficial to PA. Images were taken at 5 cm above the popliteal fossa crease where the TN and CPN have just started diverging. Simulated needle path to reach the sciatic nerve in the popliteal fossa through the posterior approach. The sciatic nerve (ScN) is seen in the adipose tissue of the popliteal fossa between bicep femoris muscle (BFM) laterally and the semitendinosus and semimembranosus muscles medially JVP/PM/OWN/MB 2014 Spectrum Medical Group So. Anesthesiology Division Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 TAP: surgery involving mid abdominal area such as hysterectomy, laparoscopic colectomy; may consider placement of catheters. May be considered for inguinal hernia repair. The aim of a TAP block is to deposit local anaesthetic in the plane between the internal oblique and transversus abdominis muscles targeting the spinal nerves in this plane. The innervation to abdominal skin, muscles and parietal peritoneum will be interrupted. If surgery traverses the peritoneal cavity, dull visceral pain (from spasm or inflammation following surgical insult) will still be experienced. Image of the abdominal wall. E0: external oblique, IO: internal oblique, TA: transversus abdominis Correct local anaesthetic deposition in the transversus abdominis plane. JVP/PM/OWN/MB 2014 Spectrum Medical Group So. Anesthesiology Division Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 Ankle Block: 1. The five nerves supplying the foot can be blocked at the ankle. Elevate the foot on a pillow to provide easy access to both sides of the ankle. 2. You will need: 2% lidocaine 25-35mls 25g 1 ½ needle on control top syringe 3. At the superior border of the malleoli, the deep peroneal nerve is situated between the anterior tibialis tendon and the extensor hallucis longus tendon, which are easily palpable with the dorsiflexion of the foot and extention of the great toe. Insert a 1.5 inch needle just lateral to the anterior tibial artery between the two tendons until contacting the tibia and then withdraw the needle while depositing 5 to 10 ml of 2% lidocaine. 4. Then, inject 10mls of 2% lidocaine subcutaneously across the anterior surface of the tibia, from malleolus to malleolus. This will block the superficial peroneal nerve laterally and the saphenous nerve medially. 5. To block the posterior tibial nerve, insert a needle posterior to the medial malleolus, directed toward the inferior border of the posterior tibial artery. A paresthesia may be noted in the sole of the foot. Withdraw the needle 1 cm from the point of bony contact and inject 5 to 10mls of 2% lidocaine in a fan-shaped area. 6. Block the sural nerve by inserting the needle midway between the Achilles tendon and the lateral malleolus, directing it toward the posterior surface of the lateral malleolus. After contacting the bone, withdraw the needle and inject 5mls of 2% lidocaine. 7. Ultrasound guided ankle block can be performed with a small linear high-frequency probe. The posterior tibial, sural and deep peroneal nerves are easily identified as hyperechoic structures along their typical anatomical distribution. The saphenous nerve is more easily identified at the same level of the knee. The common peroneal nerve is best blocked by a field block as the terminal nerves at the level of the ankle are not easily visualized. Complications of lower extremity blocks include epidural blockade with potential Sympathectomy (psoas block), intravascular injection, inadvertent arterial puncture, neural trauma and infection. (Handbook of Clinical Anesthesia Procedures of the Massachusetts General hospital) JVP/PM/OWN/MB 2014 Spectrum Medical Group So. Anesthesiology Division Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 Paravertebral block: 2. T4-T6 for chest wall surgery. Specifically for TAVR - 3 levels nerve roots of T4,5 and 6. 3. T3 (T4 NR) for mastectomy 4. L1 (T12, L1 NR) for inguinal hernia Thoracic or Lumbar Paravertebral Block Technique: Place the patient in the sitting position for optimization of anatomic landmarks as well as for patient comfort. Mark anatomy: Mark head of spinous process accordingly: 1. T3 mastectomy 2. T4 thoracoscopy 3. L1 open inguinal hernia repair Mark patient 2.5cm lateral to midline level of spinous process Raise a skin wheal at this point. Extend wheal ~1 cm cranially/caudally in case need to change insertion site Approach: Perpendicular to skin Insert 8 cm 22g Touhy needle; continue until transverse process is encountered Thoracic PVB: Once transverse process found, withdrawn Touhy slightly and change angle to “sneak” just under transverse process Advance to depth 1 cm deep to where transverse process originally encountered A subtle pop may be appreciated as the needle tip traverses the superior costotransverse ligament. Some advocate using a loss-of-resistance technique as an alternative to localizing the paravertebral space. After gentle aspiration for CSF, air or blood, local anesthetic can be administered or a paravertebral catheter can be threaded into the space. Lumbar PVB: Once transverse process is found, redirect needle approach above or below the transverse process and advance approximate 0.5-1cm deep and inject one half of the total volume of local anesthetic. Withdraw needle, and redirect above or below and repeat. Loss of resistance is more subtle and may not be appreciated at all. Complications: specific to this block include pneumothorax, possible retroperitoneal injection(kidney), intrathecal, epidural and intravascular injection Hints: Transverse process usually found at depth 2.8-4 cm. Do not search >4-5 cm, risk of pneumothorax Probably don’t go above transverse process with Touhy->increased risk of pneumothorax, except lumbar Painful for patient when periosteum of transverse process touched with Touhy JVP/PM/OWN/MB 2014 Spectrum Medical Group So. Anesthesiology Division Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 Think critically before doing a bilateral paravertebral block for bilateral mastectomy (maybe only do in patients with favorable anatomy due to ptx risk). Block Type Femoral Pop fossa/high sciatic Paravertebral TAP Interscalene/ Supraclavicular Technique Single shot Stimuplex 2 inch stimulating needle (occasionally, 4 inch) Chlorhexidine prep Sterile marking pen Large tegaderm 3cc syringe Blunt needle 25g 1.5 inch needle 1% lidocaine 5mls 60cc syringe Control syringe Stop cock Extension tubing Sterile ultrasound gel pack Sterile gloves Stimuplex 2 inch stimulating needle (occasionally, 4 inch) Chlorhexidine prep Sterile marking pen Large tegaderm 3cc syringe Blunt needle 25g 1.5 inch needle 1% lidocaine 5mls 60cc syringe Control syringe Stop cock Extension tubing Sterile ultrasound gel pack Sterile gloves 22g 3.5 inch Tuohy Chlorhexidine prep Sterile marking pen 3cc syringe Blunt needle 25g 1.5 inch needle 1% lidocaine 5mls 60cc syringe Control syringe Stop cock Extension tubing Sterile gloves Technique Catheter Nerve block tray Contiplex Nerve Block Set(2 inch or 4 inch) 25g 1.5 inch needle 60cc syringe Control syringe Stop cock CHG tegaderm (7x8.5 cm) StatLock Sterile marking pen Steri strips Ultrasound Medications Yes *(see below) Ropivacaine 0.2% with Clonidine 100mcg Volume: 30-40cc Nerve block tray Contiplex Nerve Block Set(2 inch or 4 inch) 25g 1.5 inch needle 60cc syringe Control syringe Stop cock CHG tegaderm (7x8.5 cm) StatLock Sterile marking pen Steri strips Yes *(see below) Epidural tray Styletted catheter Sterile marking pen 60cc syringe Control syringe Stop cock Extension tubing Steri strips No ** (see below) 22g 3.5 inch Tuohy Chlorhexidine prep Sterile marking pen Large tegaderm 60cc syringe Control syringe Stop cock Extension tubing Sterile ultrasound gel pack Sterile gloves Most likely this will be bilateral catheters Epidural tray 18g 3.5 Tuohy Epidural catheter (2)CHG tegaderm (7x8.5 cm) 60cc syringe Control syringe Stop cock StatLock Sterile marking pen Steri strips Nerve block tray Contiplex Nerve Block Set 2 inch 25g 1.5 inch needle 60cc syringe Control syringe Stop cock CHG tegaderm (7x8.5 cm) StatLock Sterile marking pen Steri strips Yes Stimuplex 2 inch stimulating needle Chlorhexidine prep Sterile marking pen Large tegaderm 3cc syringe Blunt needle 25g 1.5 inch needle 1% lidocaine 5mls 60cc syringe Control syringe Stop cock Extension tubing Sterile ultrasound gel pack Sterile gloves JVP/PM/OWN/MB 2014 Other drug/concentrations should be discussed with staff on a case by case basis. Ropivacaine 0.2% with Clonidine 100mcg Volume: 40cc OR Ropivacaine 0.5% and clonidine 100mcg, total volume 20cc may be considered, depending on patient’s weight. Other drug/concentrations should be discussed with staff on a case by case basis. Lumbar paravertebral: Ropivacaine 0.2% Clonidine 100mcg Volume: 30cc (L1 15cc above and below) Thoracic paravertebral: Mastectomy Ropivacaine 0.2% with clonidine 100mcg Volume: 15cc below T3 (Bilateral, mix total volume 30cc; 15cc each side) TAVR Ropivacaine 0.5% with clonidine 100mcg Total volume 20cc (3 level injection, TVP T4, 5 and 6. Inject 5cc below TVP at each level) Ropivacaine 0.2% with Clonidine 100mcg Volume: 40cc (20cc bolus each side) Ropivacaine 0.5% and clonidine 100mcg, total volume 20cc may be considered, depending on patient’s weight. Other drug/concentrations should be discussed with staff on a case by case basis. Yes *(see below) Ropivacaine 0.2% Clonidine 100mcg Volume: 20cc Other drug/concentrations should be discussed with staff on a case by case basis. Spectrum Medical Group So. Anesthesiology Division Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 *For all of these blocks, a nerve stimulator may be considered. ** Ultrasound may be considered (staff dependent). JVP/PM/OWN/MB 2014 Spectrum Medical Group So. Anesthesiology Division Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 Link: http://nysora.com/ JVP/PM/OWN/MB 2014 Spectrum Medical Group So. Anesthesiology Division Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 Link: http://nysora.com/ JVP/PM/OWN/MB 2014 Spectrum Medical Group So. Anesthesiology Division Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 M – TURBO ULTRASOUND SYSTEM QUICK GUIDE 1. 2. 3. 4. 5. 6. 7. 8. Order entry “US Anesthesia Nerve Block MMC” in EPIC Power (ON/OFF) – Upper left corner of machine Patient information Press Patient key on right side Select Worklist Highlight patient name with cursor Click “Select” Select 2D to return to US screen Gain (Brightness of image). Use the three gray dials on lower left side: Near – top half of screen Far – bottom half of screen Overall Gain – overall image Auto Gain – adjusts entire image. Located to the right of the dials. Color image – lower right corner. Allows for color imaging Block completed Save Images to PACS – lower right hand corner of the touch pad. End patient by selecting “patient” and click “new/end” from upper buttons JVP/PM/OWN/MB 2014 Spectrum Medical Group So. Anesthesiology Division Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 Recommended Max dose 1. 2. 3. Lidocaine/Mepivacaine 5mg/kg, 7 mg/kg with epi Bupivacaine/Ropivacaine 3 mg/kg regardless Continuous infusion Adults: Bupivacaine 0.5mg/kg/hr, Ropivacaine 0.6mg/kg/hr Pediatric: Bupivacaine 0.2-0.3 mg/kg/hr Prevention of LAST (Local Anesthetic Systemic Toxicity) Use minimal effective dose Use safer local anesthetic (ropivacaine instead of bupivacaine) Watch for unintentional intravascular injection 1. Immobile needle 2. Test dose after each needle repositioning 3. Aspirate before injection 4. Slow incremental bolusing Communicate frequently with patient Classical clinical presentation of systemic toxicity Major cardiovascular toxicity usually requires about 2-3 times higher concentration of local anesthetic in blood than concentration that produces seizures (so patient can warn you before) Treatment of LAST FOLLOW ASRA GUIDELINES FOR THE TREATMENT OF LAST Dose: Bolus 1.5ml/kg IV over 1 minute (~100ml); then start infusion of 0.25ml/kg/min (~18ml/min) Repeat bolus once or twice for persistent CV collapse Double infusion rate to 0.5ml/kg/min if BP remains low Continuous infusion for at least 10 minutes after CV stability *Intralipid 20% emulsion is stored in the bottom draw of each Block Cart (Bean and PACU 20) JVP/PM/OWN/MB 2014 Spectrum Medical Group So. Anesthesiology Division Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 JVP/PM/OWN/MB 2014 Spectrum Medical Group So. Anesthesiology Division Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 Link: http://www.asra.com/ JVP/PM/OWN/MB 2014 Spectrum Medical Group So. Anesthesiology Division Anesthesia Pain Management Service Guidelines for Regional Block Placement and Perioperative Management November 2014 Postoperative Management with indwelling Peripheral Nerve Catheter Needle/Catheter Contiplex Nerve Block Set 2 inch: Catheter is closed tip 20g, same markings as the epidural catheter we use. 2 inch - 10cm mark at hub is when the catheter is at the needle tip 4 inch – 15cm mark at hub is when the catheter is at the needle tip Bolus Dose Refer to page #6 Securing Catheter to skin Consider using steri strips to secure catheter to skin Dressing: Tegaderm CHG 7x8.5 cm StatLock Peripheral Nerve Catheter Infusion order sets in EPIC Anes Superificial Nerve Block for Post op Pain 1. High Sciatic 2. Sciaitic Popliteal Fossa 3. Femeral 4. Brachial Plexus 5. TAP Anes Deep Peripheral Nerve Catheter Infusion (has the same anticoagulation warning as epidurals) 1. Paravertebral 2. Lumbar Plexus Perferred solution/rate 1. Ropivacaine 0.2% at 8ml/hr 2. May consider increasing concentration of ropivacaine to 0.3% and/or increasing the rate 3. An increase rate may cause leaking at the insertion site. Consider reducing the infusion rate by increasing the concentration for pain. Inadequate analgesia in PACU Consider bolusing catheter with10cc 0.5% ropivacaine (discuss with attending first) Consider increasing rate Consider increasing ropivacaine concentration to 0.3% Consider IV PCA or oral analgesics Non opioid agents Addition Modalities/ Adjuvant therapy IV PCA Ketamine Phantom limb pain s/p AKA/BKA such as: (discuss with attending first) 1. Anticonvulsants 2. Tricylic antidepressants Postoperative Management of Single Shot Block 1. 2. 3. 4. 5. 6. Discuss with the surgeons, patient and nursing staff the expected duration of the regional block. Provide a pain management protocol to avoid severe pain when the block wears off. Consider IV PCA Oral analgesics Non opioid agents Consider Ketamine for chronic opioid tolerate patients Trouble - shooting mechanical/pump problems See Anesthesia Pain Management Service Guidelines for Thoracic Epidural Analgesia Placement and Perioperative Management JVP/PM/OWN/MB 2014 Spectrum Medical Group So. Anesthesiology Division