SHOULDER ASSESSMENT – TESTING
advertisement

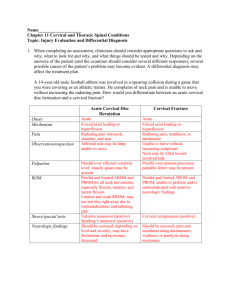
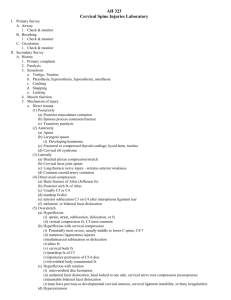
Testing 1 CERVICAL AND THORACIC SPINAL ASSESSMENT Testing If significant physical finding indicates possible nerve involvement, immobilization and immediate transportation to the nearest medical facility are warranted, regardless of whether a total assessment is complete. Range of Motion Tests —Assessment potentially includes active ROM, passive ROM, and resisted ROM —Bilateral comparison should be performed Cervical flexion 80–90 Cervical extension 70 Lateral cervical flexion (left and right) 20–45 Cervical rotation (left and right) 70–90 Manual Muscle Tests Muscle Grading Normal = 5 Full strength Good = 4 Slight weakness Fair = 3 Noticeable weakness; + pain Poor = 2 Gravity only; – pain Trace = 1 Without gravity Zero = 0 No contraction Muscles Anterior neck flexors Anterolateral neck flexors Posterolateral neck extensors Upper trapezius Stress and Functional Tests Brachial plexus traction test Cervical compression test Spurling test Cervical distraction test Shoulder abduction test Vertebral artery test First thoracic nerve root stretch Neurologic Tests Babinski test Oppenheim test Hoffman’s sign Dermatomes (normal, hyperesthesia, hypoesthesia, anesthesia, superficial tactile sensation, superficial pain sensation) o C2 – occipital protuberance o C3 – supraclavicular fossa Testing 2 o C4 – acromioclavicular joint o C5 – lateral upper arm o C6 – lateral forearm, thumb, 1st finger o C7 – middle finger o C8 – 4th and 5th fingers, medial forearm o T1 – medial upper arm Myotomes o C1-C2 – neck flexion o C3 – lateral neck flexion o C4 – shoulder elevation o C5 – shoulder abduction o C6 – biceps flexion, wrist extension o C7 – triceps extension, wrist flexion o C8 – finger flexion o T1 – finger abduction Reflexes o Biceps (C5, C6) o Brachioradialis (C5, C6) o Triceps (C7, C8) Vascular Carotid pulse Radial pulse Capillary refill Activity-Specific Functional Tests Performance of active movements typical of the movements executed by the individual during sport or activity participation Should assess strength, agility, flexibility, joint stability, endurance, coordination, balance, and activity-specific skill performance QUICK REFERENCE – TESTS Stress and Functional Tests Brachial plexus traction test o Examiner side flexes patient’s (pt) head to one side while applying a downward pressure on the contralateral shoulder o If test is +, increased pain, radiating through upper arm = Radiating to opposite side of lateral bending: tension of brachial plexus Radiating to same side as lateral bending: compression of cervical nerve root between vertebrae Cervical compression test o Pt is seated o Examiner standing behind pt with hands interlocking on top of pt’s head; presses down o If test is +, pain in upper cervical spine, upper extremity, or both = possible facet joint, narrowing of intervertebral foramen, or disc o Do not perform until r/o cervical fracture or instability! Testing 3 Spurling test o Examiner interlocks hands over top of pt’s head o Pt extends and laterally flexes cervical spine o Examiner applies compressive force through cervical spine o If test is +, radiating pain down arm = nerve root impingement (narrowing neural foramina) Cervical distraction test o Pt is supine and relaxed o Examiner: one hand under occiput; other hand on top of forehead to stabilize head o Examiner applies traction to head (distract cervical spine) o If test is +, relieve/decrease symptoms = compression of facet joint/stenosis Shoulder abduction test o Pt is seated or standing o Pt is instructed to actively abduct arm so hand is resting on top of head o If test is +, decreased tension on involved nerve root = herniated disc or nerve root compression Vertebral artery test o Pt is supine, head off table o Examiner: support pt’s head with hands under occiput o Examiner extends and laterally flexes cervical spine o Examiner rotates head toward laterally flexed side and holds for 30 seconds (keep eyes open) o If test is +, dizziness, confusion, nystagmus, unilateral pupil change, nausea = occlusion of cervical vertebral arteries First thoracic nerve root stretch o Pt positioned with the forearm pronated to 90° o Pt instructed to abduct the arm to 90° and flex the elbow (should be no symptoms elicited in this position) o Next, pt must place their hand behind the head, fully flexing the elbow (action stretches the ulnar nerve and T1 nerve root) o If test is +, pain in the scapular area or arm = T1 nerve root pathology Neurologic Tests Babinski o Pt is supine with the eyes closed and the leg held in a slightly elevated and flexed position o Examiner: pointed object is stroked along the plantar aspect of the foot o Normal sign is for the toes to curl downward in flexion and adduction o If test is +, extension of the big toe and abduction (splaying) of the other toes = upper motor neuron lesion Oppenheim o Pt is supine o Examiner runs a fingernail along the crest of the anteromedial tibia o If test is +, the great toe extends and the other toes splay or hypersensitivity to the test = upper motor neuron lesion Hoffman’s sign Testing 4 o Examiner holds patient’s middle finger and briskly flicks the distal phalanx o If test is +, the interphalangeal joint of the thumb of the same hand flexes = upper motor neuron lesion