Carotid, Vertebral and Intracranial Artery Stent Placement
advertisement

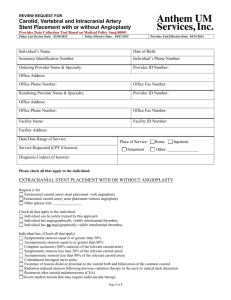
REVIEW REQUEST FOR Carotid, Vertebral and Intracranial Artery Stent Placement with or without Angioplasty Provider Data Collection Tool Based on Medical Policy Surg.00001 Policy Last Review Date: 02/13/2014 Policy Effective Date: 01/01/2015 Provider Tool Effective Date: 04/15/2014 Individual’s Name: Date of Birth: Insurance Identification Number: Individual’s Phone Number: Ordering Provider Name & Specialty: Provider ID Number: Office Address: Office Phone Number: Office Fax Number: Rendering Provider Name & Specialty: Provider ID Number: Office Address: Office Phone Number: Office Fax Number: Facility Name: Facility ID Number: Facility Address: Date/Date Range of Service: Place of Service: Service Requested (CPT if known): Outpatient Home Inpatient Other: Diagnosis Code(s) (if known): Please check all that apply to the individual: EXTRACRANIAL STENT PLACEMENT WITH OR WITHOUT ANGIOPLASTY Request is for Extracranial carotid artery stent placement with angioplasty Extracranial carotid artery stent placement without angioplasty Other (please list): Check all that apply to the individual: Individual can be safely treated by this approach Individual has angiographically visible intraluminal thrombus Individual has no angiographically visible intraluminal thrombus Individual has: (Check all that apply) Symptomatic stenosis equal to or greater than 50% Asymptomatic stenosis equal to or greater than 80% Complete occlusion (100% stenosis) of the relevant carotid artery Symptomatic stenosis less than 50% of the relevant carotid artery Asymptomatic stenosis less than 80% of the relevant carotid artery Contralateral laryngeal nerve palsy Existence of lesions distal or proximal to the carotid bulb and bifurcation of the common carotid Radiation-induced stenosis following previous radiation therapy to the neck or radical neck dissection Restenosis after carotid endarterectomy (CEA) Severe tandem lesions that may require endovascular therapy Page 1 of 2 REVIEW REQUEST FOR Carotid, Vertebral and Intracranial Artery Stent Placement with or without Angioplasty Provider Data Collection Tool Based on Medical Policy Surg.00001 Policy Last Review Date: 02/13/2014 Policy Effective Date: 01/01/2015 Provider Tool Effective Date: 04/15/2014 Stenosis secondary to arterial dissection Stenosis secondary to fibromuscular dysplasia Stenosis secondary to Takayasu arteritis Stenosis that is surgically difficult to access (e.g., high bifurcation requiring mandibular dislocation) Stenosis associated with contralateral carotid artery occlusion Stenosis that cannot be safely reached or crossed by endovascular approach Pseudoaneurysm Inability to move the neck to a suitable position for surgery Tracheostomy Stenosis or aneurysm of extracranial vertebral arteries or intracranial arteries Other (please list): Individual is at high risk for surgery (check all that apply) Individual has Congestive heart failure (NYHA Class III/IV) Left ventricular ejection fraction less than 30% Open heart surgery needed within the next 6 weeks History of recent myocardial infarction (greater than 24 hours and less than 4 weeks) Individual has severe chronic obstructive pulmonary disease Individual has unstable angina (CCS class III/IV) Other (please list): INTRACRANIAL STENT WITH OR WITHOUT ANGIOPLASTY Request is for Percutaneous intracranial artery stent placement with or without angioplasty as part of the treatment of individuals with an intracranial aneurysm. Surgical treatment is not appropriate or attempted surgery was unsuccessful Standard endovascular techniques (coiling) are inadequate to achieve complete isolation of the aneurysm because of anatomic considerations which include (please check all that apply) Wide-neck aneurysm (4 mm or more) Sack-to-neck ratio less than 2:1 Other (please list): This request is being submitted: Pre-Claim Post–Claim. If checked, please attach the claim or indicate the claim number I attest the information provided is true and accurate to the best of my knowledge. I understand that the health plan or its designees may perform a routine audit and request the medical documentation to verify the accuracy of the information reported on this form. _____________________________________________________________ Name and Title of Provider or Provider Representative Completing Form and Attestation (Please Print)* Date *The attestation fields must be completed by a provider or provider representative in order for the tool to be accepted Anthem Blue Cross is the trade name of Blue Cross of California. Anthem Blue Cross and Anthem Blue Cross Life and Health Insurance Company are independent licensees of the Blue Cross Association. ® ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross name and symbol are registered marks of the Blue Cross Association. For some plans utilization review services are provided by Anthem UM Services, Inc., a separate company. Page 2 of 2