Lipoma-Liposarcoma
advertisement

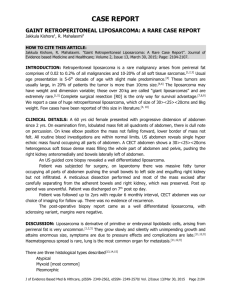
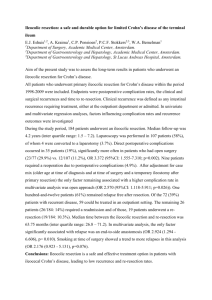
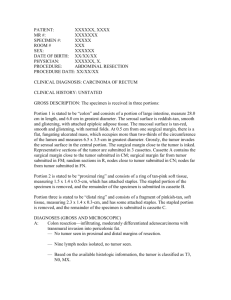
Atypical Lipoma/Well Differentiated Liposarcoma, dedifferentiated to a Myxoid Liposarcoma Liposarcomas are one of the most common soft tissue sarcomas of adult life. Many subtitles exist and exact diagnosis is often difficult. Characteristics of Liposarcoma: Liposarcomas are usually deeply located. (Lipomas usually occur in superficial, soft tissue). They rarely if ever develop from benign lipomas. Proper sampling of the gross tumor is critical for proper diagnosis. Liposarcomas occur rarely in children. Liposarcomas are less well defined than lipomas. Liposarcomas may become very large. Atypical Lipoma/Well Differentiated Liposarcoma/Atypical Lipomatous Tumor Characteristics are: Usually does not metastasize but often recurs Often deep and large May have bizarre stromal cells 50% in the extremities may recur Small % over time dedifferentiate to a high grade malignant tumor After 7-8 years, as long as 17-20 years after original dx 17% mets, 28% die of their disease I - 3022-03, 3022-04 This 65 year old white male banker and scratch golfer was seen on 2-3-1995 with a large soft tissue mass in his left posterior thigh present for many months which had become painful. On examination the left thigh demonstrated a huge soft tissue mass with increased circumference of 12 cm over that of the right thigh. These radiographs of the involved thigh demonstrate a large, soft, tumor mass which is less dense radiographically than the adjacent muscle. This less dense mass indicates the presence of fat and suggests the diagnosis of an intramuscular Lipoma. This x-ray can be considered a ”poor man’s” MRI in detecting a fatty tumor. However, it cannot differentiate between a benign or malignant fatty tumor. The underlying bone appeared normal. He has unrelated degenerative arthritis of both hips. 3022-02, 3022-06 These MRI’s demonstrate a large soft tissue tumor mass compatible with the diagnosis of an intramuscular Lipoma. These MRI findings, are often found in benign Lipomas because of the obvious fat and is unusual in Liposarcomas. Chest x-ray was clear. He also had atrial fibrillation and coronary artery disease but was in good general health. 3022-07, 3022-08 The soft tissue tumor mass considered to be a benign Lipoma was resected. It measured 29 x 24 x 6 cm and weighed 1.5 kilograms. Multiple sections, throughout the mass, showed areas of fat necrosis. The final diagnosis by the Pathologist was Lipoma with areas of organized fat necrosis. (1995) Images, 4, 5, 6 These histosections made from the tumor mass demonstrate a fairly typical Lipoma although some lipoblastic pleomorphism was found indicating this could be an atypical Lipoma. Multiple sections showed bizarre stromal cells were present which strongly suggest an Atypical Lipoma/well differentiated Liposarcoma. In either case, Lipoma or atypical Lipoma, metastasis does not occur but recurrence particularly in atypical Lipoma is not uncommon. Several days after surgery, the patient did develop extensive cellulitis in the posterior thigh adjacent to the operative incision. Needle aspiration of the cellulitis was negative. Pus was not found. An organism was not obtained. The patient was placed on oral antibiotics and over several weeks the cellulitis subsided. The patient then did very well for many years. II -Images 12, 14, 22 Ten years later in May of 2005, at Warren General Hospital in Warren PA., a resection of the large recurrence of the Lipoma was performed in a hospital close to his home in Pennsylvania. These sections from this recurrence do show some cells with bizarre nuclei and probably represents recurrent Atypical/well differentiated Liposarcoma. III - Img_6604, Img_6605 However, four years later in 2009, the second resection of an enormous, soft tissue recurrence which had rapidly developed in his posterior left thigh. Chest x-ray was normal. These two MRI’s demonstrate the enormous recurrence. Histosections of the biopsy of the rapidly growing recurrence demonstrated a myxoid Liposarcoma, medium grade quite different from earlier biopsy interpretations. Images 24, 25, 29 In March of 2009, several months after the latest biopsy, a marginal excision of the myxoid Liposarcoma was performed at RPCI including removing portions of the gluteus maximus, gracilis and including neurolysis of the sciatic nerve. This mass was 45 cm. in maximal diameter and weighed 6100 grams. The operative incision extended from his buttock to the popliteal space. Because all of the adjacent soft tissue was not removed at this resection, biopsy of residual tissues demonstrated myxoid Liposarcoma. Thus only a marginal resection was performed. He was given 70.4 Gy of adjuvant radiation because of the still present Liposarcoma in the patient. Summary of treatments 1. 2. 3. 4. Initial resection 1995-Atypical Lipoma/Well differentiated Liposarcoma Resection of first recurrence in 2005- same diagnosis Resection of second recurrence in 2009- Dedifferentiated Myxoid Liposarcoma Post op radiation 70.4 Gy of adjuvant radiation Phone call to the patient on 8-25-2011 indicates that he is 82 years old and “free of tumor.” On the phone, he told me his posterior thigh was markedly scarred by prior surgery but as far as he knows is “without evidence of recurrence.” However, he has persistent pain now, 10-2011, behind his knee and leg thought to be due to the radiation. However, he continues to have trouble with his leg. Chest x-rays every 6 months have been normal. He has retired from banking and feels good. His hips are bad and he could only walk one block easily. Learning Issues: There are several possible scenarios in this case. We believe the initial diagnosis in 1995 because of its deep location in the posterior thigh, its large size and the bizarre appearance of the stromal cells that the most likely diagnosis was atypical Lipoma/well differentiated Liposarcoma. If tissue blocks from the initial 1995 surgery were available an MDM2 stain could have confirmed the diagnosis of Atypical Lipoma/well differentiated Liposarcoma. This lesion recurs often but does not metastasize. Ten years later in 2005, the lesion recurred and was resected in a hospital near his home in Warren, Pennsylvania. The diagnosis of this tissue removed remains atypical Lipoma/well differentiated Liposarcoma in our opinion. In 2009, four years after the resection of the first recurrence, a massive recurrence occurred, which on biopsy revealed a fully malignant myxoid Liposarcoma. This indicated that the lesion had dedifferentiated to a fully malignant tumor. A marginal resection of this enormous tumor was performed at RPCI and he was given heavy, local post op radiation. Radiation is not usually very effective against Liposarcoma. Thus, 16 years after his first treatment and two years after his marginal resection of the myxoid Liposarcoma he remains liable to further recurrence, metastasis or the development of radiation Sarcoma. He needs further follow up studies. CT scan of his lungs and MRI of his thigh are being planned.