bone tumours
advertisement

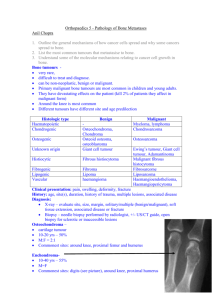
Bone tumours- presentation pain swelling pathologic fracture General characteristics malignant primary bone tumours are rare- in total only 6 mln population/ year although rare they are highly aggressive all present with mechanical pain followed later by sweling delays in diagnosis are common X- Ray feature ssuggestive of bone tumours include bone destruction new bone formation soft tissue swelling periosteal elevation 1 Metastases are blood-borne and usually arise first in the lungs Giant cell tumour (Osteoclastoma) young adults location: epiphysis (especially the knee) X Ray: osteolytic and slowly progressive although benign histologically they may behave in a biologically malignant way and metastases occur in 1% treatment: detailed and thorough curettage Ewing’s sarcoma children location: long bones ( typically the diaphysis ) and limb girdles X Ray: large soft- tissue mass with concentric layers of new bone formation (“onion-peel” sign) t: 11-22 present 2 chemiotherapy, resection and limb salvage surgery or radiotherapy cures about half poor prognosis due to large volume or metastatic disease at presentation Osteosarcoma adolescents arises towards the end of long bones (typically the knee) in the metaphysis secondary osteosarcomas may arise in bone affected by Paget’s disease or after irradiation X Ray: bone destruction or new bone formation with periosteal elevation treatment: chemiotherapy followed by surgical resection vigorous treatment of metastatic disease is worthwhile 3 Chondrosarcoma may arise de novo from malignant transformation of chondromas middle age slowly icresing mass occasionally causing pressure symptoms X Ray: “cotton wool” calcification treatment: only surgery- no response to chemiotherapy, radiotherapy inadequate surgery=> not only local recurrence but often a higher grade of malignancy Malignant fibrous histiocytoma rarest of all primary bone tumours middle age often the site of previous bone abnormality (eg. bone infarcts) tratment: as for Osteosarcoma 4 Chordomas arise from notochord remnants in the spine most common in sacrum often large size before diagnosis may present with neurological signs (bladder, bowels) treatment: radical surgical excision is mandatory for cure Osteoid osteoma males 10-25 years most common in long bones X ray: local cortical sclerosis treatment: local excision Chondroma cartilaginous tumour, may arise from bone surfaces or within the medulla (enchondromata) present with local swelling or fracture 5 Osteochondroma (autosomal dominant) the commonest of benign tumours arises from the metaphyseal areas of bone as rounded swelling Both chondromata and osteochondromata rarely undergo malignant change so treatment is rarely indicated. Suspect malignancy if pain develops! 6