CUSP for Safe Surgery (SUSP) Annual Report
advertisement
 Annual Report")
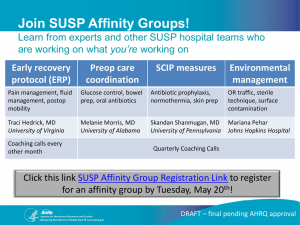
CUSP for Safe Surgery (SUSP) Option Year One Report A Project of: Johns Hopkins University Armstrong Institute for Patient Safety and Quality American College of Surgeons University of Pennsylvania Contract No: HHSA2902010000271 Dates: September 2012 – August 2013 Disclaimer: This report was developed with data collected and analyzed under contract with the Agency for Healthcare Research and Quality (AHRQ). Table of Contents Executive Summary....................................................................................................................................... 3 Introduction and Objectives ......................................................................................................................... 4 Methods ........................................................................................................................................................ 4 Hospital Recruitment ................................................................................................................................ 4 Recruitment Plan .................................................................................................................................. 5 SUSP Portal and Database ........................................................................................................................ 5 Safety Climate Measurement (Hospital Survey on Patient Safety [HSOPS]) ............................................ 5 Surgical Site Infection Rate Reporting ...................................................................................................... 6 Ethnographic Methods and Process ......................................................................................................... 6 Results ........................................................................................................................................................... 6 State and Hospital Recruitment ................................................................................................................ 6 Safety Climate (HSOPS) Data .................................................................................................................... 8 HSOPS Data Collection Method and Interim Participation Rates ......................................................... 8 HSOPS Interim Results .......................................................................................................................... 8 Surgical Site Infection Data ....................................................................................................................... 9 Ethnographic Data and Lessons-Learned................................................................................................ 11 A Lesson Re-Learned: The Adaptive Work of Culture Change is Challenging ..................................... 11 The NPT Needs to Enable Horizontal Learning ................................................................................... 11 Teams Want Flexibility within a Defined Program Structure ............................................................. 11 The Path Forward........................................................................................................................................ 12 Reverse Innovation: Learning from International SUSP Sites ............................................................. 12 Conclusion ................................................................................................................................................... 12 References .................................................................................................................................................. 14 Appendix A: Sample Ethnography Site Visit Memo ................................................................................ 15 Executive Summary Background Nearly 50 million people have surgery each year in the U.S. Approximately one million develop serious complications and over 150,000 patients die within 30 days. Healthcare acquired infections are among the most common complications in surgery patients. These complications impart an enormous burden on patients, their families, employers, and society. While the cost of caring for surgical patients without complications varies among hospitals, any single complication can double or triple the costs of care. Inhospital complications are also strongly associated with hospital readmission. As such, there is a clinical and economic imperative to prevent surgical harm. A collaborative multifaceted approach is needed to reduce these complications. The Department of Health and Human Services’ National Action Plan to Reduce Healthcare-Associated Infection provides a national level plan; yet healthcare is local. Surgical safety requires a strategy to engage front-line clinicians and hospital leaders; utilize performance measures clinicians believe are valid; adapt methods based on local context to ensure patients receive evidence-based therapies; and implement a process to improve culture and teamwork and learn from mistakes. The Agency for Healthcare Research and Quality (AHRQ) has funded a National Project Team (NPT) with representatives from the Johns Hopkins University Armstrong Institute for Patient Safety and Quality in partnership with the American College of Surgeons, the University of Pennsylvania and the World Health Organization to design, disseminate and evaluate CUSP for Safe Surgery (SUSP), a surgical safety program that provides shape to this strategy. Participation All acute care hospitals across the United States and Puerto Rico are eligible to participate in SUSP. Recruitment began in the project’s base year, and is ongoing. The recruitment plan has evolved to enable broader participation in the project over time. To date, a total of 12 coordinating entities and 159 hospitals have enrolled in the SUSP project. 11 hospitals enrolled during the base year, and 148 hospitals enrolled during option year one. Recruitment for cohort four was opened in August 2013. Conclusions The NPT is learning how to locally tailor and disseminate SUSP in a complex healthcare environment with frontline clinicians and coordinating entities that are more overextended than ever before. Currently there is insufficient data from hospital teams to draw conclusions about the impact of SUSP on SSI rates, but the NPT anticipates that SSI data submission rates will improve over the second option year. By tapping the intrinsic motivation of frontline staff in perioperative units across the country, SUSP will yield powerful stories, meaningful data, and safer care for surgical patients. 3|CUSP for Safe Surgery Option Year One Report Introduction and Objectives Since 2009, over 1,000 hospitals have joined On the CUSP: Stop BSI to eliminate central line-associated blood stream infections (CLABSI), a hospital-associated infection once perceived as inevitable, in their intensive care units.1 Their indisputable success shows that engaged teams can transform care when they own a problem, apply proven improvement strategies, and learn from each other.2 Surgical teams at the Johns Hopkins Hospital have applied these principles in their perioperative area, and reduced their surgical site infection (SSI) rates by 33 percent.3 Yet duplication of this success at a national scale is not guaranteed. Surgical teams have exceedingly complex social and political structures enmeshed in a rich and noble history, full of traditions and hierarchy, comprised of many sub-teams. The science for surgical harm prevention is less mature than CLABSI prevention. The measures are noisy. Yet the need could not be greater: Quick fixes have not been effective, and preventable harm in surgical patients continues seemingly unabated. The SUSP NPT has tapped the collective wisdom of quality improvement experts, diverse stakeholder groups, and clinicians to develop and implement SUSP as an innovative national project to reduce surgical site infections and other surgical complications. The NPT aims to create a clinical community: An enduring network of organizations accountable for efficient and effective sharing of knowledge, and supportive of improvement and innovation. This community includes a vertical core of national experts and project leaders, including faculty from the Armstrong Institute for Patient safety and Quality, the American College of Surgeons, the University of Pennsylvania, and the World Health Organization; and a horizontal core of peer hospitals and coordinating entities (CEs), such as state hospital associations and Hospital Engagement Networks (HENs). The NPT is learning how to tailor and disseminate this surgical safety project in a complex healthcare environment with frontline clinicians and CEs that are more overextended than ever before. The NPT is eager to tell its story, enable AHRQ to assess project progress, and work with partners including AHRQ to improve the project. Through the production of this report, the NPT seeks to achieve three goals: 1. Describe SUSP project recruitment and evaluation methods for key project outcomes 2. Provide interim available data on recruitment, safety culture, SSI and ethnography site visits 3. Identify opportunities to adapt and improve the project during remaining option periods Methods Hospital Recruitment The recruitment plan has evolved over time to enable broader participation in the project. As in other national collaborative projects, enrollment is open for a specified period of time (in this case 2 months per recruitment period) and hospitals enrolling during the same period are organized into cohorts. In brief, participation in cohorts one through three was limited to hospitals reporting SSI for colorectal surgeries to ACS-NSQIP and/or NHSN. Beginning with cohort four, all interested acute care hospitals across the US and Puerto Rico, including those currently enrolled in SUSP, may enroll teams from any surgical service line (e.g., general, orthopedic, neurosurgeries, etc). 4|CUSP for Safe Surgery Option Year One Report Recruitment Plan Recruitment began in the project’s base year, and is ongoing. The NPT designed SUSP so that participating hospitals could initially focus on SSI reduction in colorectal surgery. The NPT hypothesized that hospital teams, through implementation of effective improvement methods, could demonstrate significant SSI reduction due to relatively high infection rates following colorectal surgery. Hospital teams could then apply tested improvement methods to other service lines and surgical complications. NPT members also felt strongly that they should minimize over-extended hospital teams’ data collection burden, and began developing a system to transfer colorectal SSI data from existing databases into the SUSP database. Due to this data transfer plan, the NPT initially instructed CEs to recruit NSQIPparticipating hospitals into the first SUSP cohort, and encouraged all hospitals to join in subsequent cohorts. This approach was designed to ensure the acquisition of valid baseline data from hospital teams, and gave the NPT time to develop minimally burdensome data requirements for subsequent states and teams that were not NSQIP participants. Beginning with the second SUSP cohort, the NPT opened project recruitment to hospitals submitting colorectal SSI data to the Centers for Disease Control and Prevention (CDC) National Healthcare Safety Network (NHSN). The NPT learned during the base year that some hospital teams enrolled in SUSP were already applying project concepts to reduce SSI in other types of surgical procedures (e.g. orthopedic or neurosurgeries). The NPT believes, as these teams demonstrated, that SUSP is agnostic to surgical line, and has encouraged hospital teams performing any type of surgery to join cohort four. As a result, the NPT expects to enroll a larger number of hospitals into cohort four and subsequent cohorts. SUSP Portal and Database The NPT worked with a vendor (CECity.com, Inc.) to develop the SUSP project portal as a central resource for project content and data, and a link to a project-specific social networking site. The portal includes the SUSP project database, a central repository of data that is used to support project-related quality improvement initiatives and evaluate the impact of SUSP initiatives on perioperative safety climate and SSI rates. Participating hospitals or their designated representative, such as the CE, submit hospital safety climate and SSI data to the database for analysis and reporting. The results presented in this report are based on analyses conducted with data drawn from the database in July 2013. Safety Climate Measurement (Hospital Survey on Patient Safety [HSOPS]) An important early step in the CUSP process includes systematically measuring or in some other way understanding the Safety Climate of the work area in which improvement efforts are unfolding. Baseline data regarding perioperative Safety Climate were collected using the HSOPS survey, the publically available survey instrument developed by Westat under funding from AHRQ (Sorra & Neiva, 2004). The survey measures 10 dimensions of Safety Climate, 3 self-rated outcomes related to safety climate (e.g., overall patient safety grade, overall perceptions of patient safety), and also demographic data. The survey, while given to individuals within the unit, is designed to measure group-level perception of safety climate within respective work areas, therefore, data were aggregated to the work area level-of-analysis for reporting purposes and interim analyses. Participating teams could contribute 5|CUSP for Safe Surgery Option Year One Report HSOPS data in one of two ways: (1) collect real-time HSOPS data using the online SUSP data collection platform, or (2) upload previously collected HSOPS data if collected in the previous 12 calendar months and were available at the individual respondent level. Surgical Site Infection Rate Reporting Participating hospitals may submit SSI data from NHSN, NSQIP or both. Adjusted (six-month aggregate) and unadjusted (monthly aggregate) data for superficial, deep and organ space SSI can be transferred into the SUSP database. For NHSN data, either the CE or hospital administrator exports SSI data out of NHSN and imports data into the SUSP project database. For NSQIP data, ACS transfers SSI data to the NPT, who then imports it into the SUSP project database. SUSP project SSI data reporting mirrored the successful data reporting process utilized in the On the CUSP: Stop BSI project. Once the data is submitted, both CEs and hospital administrators are able to view their data in the SUSP registry through both the application (app) performance monitor as well as the network performance monitor. Both of these views allow the CE and hospital administrators to the monitor the numerator (infections) and denominator (cases) of their hospitals. They can also view trend graphs, peer comparators, and percentile rankings. Web-based reports are available to participants to provide current information to be shared with SUSP teams. The NPT encourages hospital teams to share SSI data internally, e.g. posting data in surgical unit break rooms. Ethnographic Methods and Process Ethnographic research is a method for addressing the tension between a plan and its implementation. The ethnographic team of social scientists from the University of Pennsylvania has focused on studying how frontline workers make sense of their work world and create the patterns discovered through statistical analysis of aggregated quantitative data sets. The qualitative component of the SUSP project is aimed at gaining insight into how frontline providers interpret and implement the project locally at their sites. The research has captured numerous stories about successes and setbacks at creating change. The ethnography team recruited sites for ethnographic visits through a weekly listserv to CEs and have been able to accommodate all of the volunteers so far. To date, the ethnography team has visited 12 hospitals in four states. The sites include academic, critical access, and community hospitals. Three ethnographers have spent a combined 15 days of site visits overall. At each site, they observed the PreOp, OR, and PACU areas, and often the Sterile Processing Departments. In addition to their observations, they conducted over 100 individual and group interviews, ranging from 10 minutes to 2 hours. They have attended SUSP meetings, met with SUSP leadership, and interviewed individuals, from front-line personnel to executive leadership. Results State and Hospital Recruitment The SUSP project has enrolled three active cohorts (Table 1). Cohort one was enrolled during the base year, cohorts two and three were enrolled during option year one, and recruitment for cohort four was 6|CUSP for Safe Surgery Option Year One Report opened in August 2013. Project activity for cohort 4 will begin in October 2013 during option year two. To date, a total of 159 hospitals have enrolled in the SUSP project. Cohort two contains 97 hospitals from 10 coordinating entities, and includes both NSQIP-participating hospitals and those that participate in NHSN. Cohort three contains 51 hospitals from six coordinating entities. Figure 1 highlights the states from which hospitals have been enrolled into the SUSP project. To date, a total of 12 CEs have enrolled in the project and organized participating hospitals within their state or organization. Participating CEs, and the number of hospitals affiliated with each, may be found in Table 1. The Armstrong Institute is serving as CE for hospitals that did not have a participating CE at the time of enrollment. Figure 1. State Participation in CUSP for Safe Surgery, by Coordinating Entity Arkansas Hospital Association Hawaii Safer Care SUSP Collaborative Armstrong Institute for Patient Safety & Quality Iowa Healthcare Collaborative Colorado Hospital Association Maryland Hospital Association Connecticut Hospital Association Michigan Health & Hospital Association Florida Hospital Association Nevada Health Insight Georgia Hospital Association Tennessee Hospital Association Table 1. Hospital Participation in CUSP for Safe Surgery, by Coordinating Entity and Cohort Coordinating Entity Number of Hospitals Enrolled Armstrong Institute for Patient Safety and Quality 14 Arkansas Hospital Association 10 7|CUSP for Safe Surgery Option Year One Report Coordinating Entity Number of Hospitals Enrolled Colorado Hospital Association 5 Connecticut Hospital Association 6 Florida Hospital Association 7 Georgia Hospital Association 14 Hawaii Safer Care SUSP Collaborative 14 Iowa Healthcare Collaborative 13 Maryland Hospital Association 18 Michigan Health & Hospital Association 46 HealthInsight Nevada 2 Tennessee Hospital Association 10 Cohort Number of Hospitals Enrolled Cohort 1 11 Cohort 2 97 Cohort 3 51 Total Hospitals Enrolled 159 Safety Climate (HSOPS) Data HSOPS Data Collection Method and Interim Participation Rates As of July 2013, three cohorts of hospitals have participated in baseline HSOPS Survey data collection efforts. Of all hospitals participating in the project, Cohort 1 included 11 hospitals, cohort 2 included 54 hospitals, and cohort 3 included 46 hospitals who registered for the online SUSP data platform. Recruitment for cohort 4 opened in August 2013. The data collection period for cohort 1 ran between October, 2012 to December, 2012. During this period seven of the 11 hospitals uploaded their HSOPS data (64% hospital data participation rate). For Cohort 2 data collection occurred between January, 2013 to March, 2013 with 30 out of the 54 hospitals registered for the online platform contributing HSOPS data (56% hospital data participation rate). Cohort 3 data collection occurred between April, 2013 to June, 2013 with 33 hospitals submitting HSOPS data (72% hospital data participation rate). A few additional hospitals (n = 3) have requested extensions in order to upload previously collected data and we are currently supporting them in these efforts. As of July 27, 2013, HSOPS data from 5,228 individual respondents nested in 70 work-area teams across all three cohorts have been collected. Of these, 40% have contributed real-time HSOPS data that was collected using the SUSP online data platform and 60% of responses were uploaded to the online platform based upon surveys that participating teams had completed as part of their annual safety culture measurement efforts in the preceding 12-months. The mean work area survey response rate to date is 67%; that is, on average, approximately 67% of work area team members who had the opportunity to respond to the survey actually submitted responses. HSOPS Interim Results 8|CUSP for Safe Surgery Option Year One Report Interim results represent all baseline HSOPS data collected for participating hospitals in Cohorts one, two, and through July 27, 2103. In line with the AHRQ National HSOPS database, the largest proportions of respondents to date have been nurses (54%), followed by others (10%), attending/staff physicians (9%), and technicians (8%). Additionally, 49% of respondents to date have worked in their current workarea for five years or less, with 11% working in their present work-area for less than one year. Forty-six (46%) percent reported working in their present position for 10 years or less and 54% reported working 40-59 hours per week on average. Baseline composite scores for the 10 dimensions of safety climate and two composite outcome measures are displayed in Figure 2. Patterns are similar to those observed in the National AHRQ HSOPS database, with Teamwork Within Unit scoring most positively overall and Non-punitive Response to Error scoring least positively. This aligns with several qualitative themes that are emerging from the ethnographic work conducted by the University of Pennsylvania team and also anecdotally from discussions on coaching calls. Figure 2. Interim baseline HSOPS composite scores for SUSP Cohorts 1, 2, and 3 as of July 2013 Surgical Site Infection Data As of August 6, 2013, there were 159 hospitals registered in the SUSP data portal (Table 2). Of these, 43 plan to submit NHSN data, 21 plan to submit NSQIP data, and 6 plan to submit both. 89 hospitals have not declared what data source they will be submitting. Of these 159 hospitals, 32 have submitted data (26 NHSN, 6 NSQIP). The NPT believes there are several important reasons for a low SSI data submission rates. First, SSI data export from the CDC NHSN and ACS-NSQIP is complex due to the existence of SSI 9|CUSP for Safe Surgery Option Year One Report categories (superficial, deep, organ space) and the need for risk adjustment. Second, electronic data transfer requires team, hospital, and CE action, competing with many other organizational priorities. For example, CDC NHSN requires hospitals to confer rights to CEs. CEs then create the data export and upload data into the SUSP project platform. Development of the infrastructure to facilitate electronic transfer of data, including pilot testing the fidelity of the transfer process, was recently completed and the NPT anticipates data submission rates will improve. Table 2: Current summary of number of participating hospitals who have submitted NHSN and/or NSQIP data. NHSN Hospitals NSQIP Hospitals NHSN & NSQIP Undeclared Data Source Total Hospitals 43 21 6 89 159 SSI Data Available 26 6 0 0 32 Overall there is insufficient data to draw conclusions about SSI rates. Based on the preliminary data collected, the unadjusted SSI rate among the 26 NHSN hospitals is 0%, 5.07%, and 3.64%, for cohorts one, two, and three respectively (Table 3). Among the 6 NSQIP hospitals, the unadjusted SSI rate is 0%, 0%, 11.69%, for cohorts one, two, and three respectively (Table 4). It remains unclear if these SSI rates are representative of all participating hospitals. Table 3: Preliminary data on NHSN based on 638 colorectal cases Cohort 1 2 3 NHSN Colorectal Rates* (January through July 2013) 26 Hospitals 638 Colorectal Cases SSI Rate SSI Rate (SSI Events (%) # of Colorectal Cases) 0/5 0 7/138 5.07 18/495 3.64 National Average (06-08)1 5.56% Table 4: Preliminary data on NSQIP based on 638 colorectal cases Cohort 1 2 3 NSQIP Colorectal Rates* (January through July 2013) 26 Hospitals 638 Colorectal Cases SSI Rate SSI Rate (SSI Events (%) # of Colorectal Cases) 0/10 0 0/47 0 9/77 11.69 10 | C U S P f o r S a f e S u r g e r y O p t i o n Y e a r O n e R e p o r t National Average (06-08)2 11.39% Ethnographic Data and Lessons-Learned The ethnography team has provided feedback to (1) the NPT on which teaching strategies are most successful and how they can be improved; (2) providers on variation across sites and innovative practices across the visited sites; and (3) CEs on their role in the project. Their interviews are currently being transcribed; and the ethnography team has begun data coding and analysis using Nvivo software. The NPT derived lessons-learned from ethnographic observations and feedback, project calls, and discussions with CEs. A Lesson Re-Learned: The Adaptive Work of Culture Change is Challenging Hospital teams are interested in the technical components of SUSP. They want to talk about antibiotic re-dosing, the exact instruments on their clean Mayo stand, and the skin prep. The adaptive component of the project that involves “culture change” remains the most difficult part of the CUSP model for teams to grasp, manipulate, and teach or transfer. The “culture” of the place came up quite routinely in ethnographic interviews and conversations, but few teams had experienced clear success in changing the culture or agreed with each other about what needed to change. Cultural change within teams is complex, the process by which teams transform is a topic of ongoing inquiry within the ethnographic team. The NPT Needs to Enable Horizontal Learning The complex nature of SSI creates a barrier to horizontal learning, i.e. hospital teams’ ability to learn from each other’s experiences. Though participating hospitals pursue the same goals, reduction of SSI and improvement in safety climate, the approach varies widely among hospitals. For example, one hospital may identify a defect in their antibiotic dosing; another may identify a defect in the quality of skin prep. Hospital teams want to know about solutions other teams are pursuing. They want to feel that they are a valuable part of a project (no matter their size or prestige) that reaches beyond the walls of their hospital. Several teams came up with innovative ideas about how to keep up momentum and increase engagement in the project, such as keeping journals about patient safety concerns in their hospital, organizing an “ask me about SUSP” raffle, etc. (Please see examples in the attached Memo to a Site in Appendix A). The NPT is currently exploring and developing strategies to highlight and share innovative practices including the use of video messaging and assigning teams to present on monthly coaching calls. Teams Want Flexibility within a Defined Program Structure SUSP cannot be a one-size-fits-all program. SUSP teams come from perioperative areas of varying sizes, in different states of organizational change, with unique safety climates. The ethnography team has observed that SUSP project success on the hospital level depends to a great extent on the teams’ previous experience with CUSP, the existence of teams working on safety projects before SUSP, and the presence and continuity of executive support for patient safety initiatives. Hospital teams need a flexible project that they can adapt to meet their unique learning and improvement needs. Yet teams rarely have the time and resources to “figure out” how to make a project most relevant to their local context. Both CEs and hospital teams prefer prescriptive guidance regarding project tasks, e.g. not only the 11 | C U S P f o r S a f e S u r g e r y O p t i o n Y e a r O n e R e p o r t purpose of improvement tools, but also when and how to use them most effectively. The challenge, then, is to design a program that is prescriptive, but not burdensome; adaptable, but unambiguous. The Path Forward The fourth cohort of SUSP teams will begin project work in mid-October. The NPT is in the process of reorganizing SUSP content, and restructuring SUSP delivery to incorporate lessons-learned. The NPT conceptualizes SUSP as a distance learning experience, and will provide teams with a project guide that includes a high-level timeline, key milestones and course modules. Each module will contain objectives, learning resources and “homework,” such as administering HSOPS or submitting SSI data. Hospital teams may complete homework at their own pace, but will be instructed to complete tasks chronologically. The NPT is also restructuring project calls to provide additional support to CEs and hospital teams, and enable horizontal learning. The NPT has established monthly CE-level coaching calls that give hospital teams access to tailored guidance from a dedicated NPT patient safety expert. CE-level coaching calls promote hospital team accountability for completion of project work, and encourage individual team member participation and storytelling. They also provide an opportunity for NPT coaches and CEs to debrief hospital team SSI data, and close the data feedback loop that is so crucial to program success. These calls have been extremely valuable and well-received. Reverse Innovation: Learning from International SUSP Sites The NPT has partnered with the World Health Organization (WHO) to implement SUSP in international sites. The WHO has led the selection and engagement of five hospitals in Africa. Priority was given to hospitals currently working with the WHO on the development of SSI prevention guidelines, and those in the African Partnership for Patient Safety (APPS), an innovative project that builds sustainable patient safety partnerships between hospitals in the WHO African region and hospitals in other region. A key component of the WHO work is the adaptation of the SUSP protocol and tools for implementation in settings with limited resources. The WHO leads and representatives from participating African hospitals met in August 2013 in Harare, Zimbabwe to finalize project tools and toolkits and plan for the project kick off and implementation. Preliminary feedback from sites indicates that local teams are very enthusiastic and motivated and that CUSP tools retain their utility across cultures and resource levels, perhaps due to their focus on uncovering and addressing local defects. Based on preliminary analysis of local gaps and needs, new tools for implementation and monitoring are also being created with innovative focus, such as patient participation and evaluation of the cost-effectiveness of SUSP implementation in an African context. The NPT anticipates that the SUSP approach will also translate well, and expects that the project adaptation for the local context by international SUSP teams will generate invaluable lessons learned and will open the perspective for broader international scaling up. Conclusion 12 | C U S P f o r S a f e S u r g e r y O p t i o n Y e a r O n e R e p o r t The NPT is honored to work with leaders at every level of healthcare to achieve and demonstrate success at improving safety climate and reducing surgical complications. Currently there is insufficient data from hospital teams to draw conclusions about the impact of SUSP on SSI rates, but the NPT anticipates that SSI data submission rates will improve over the second option year. Nevertheless, the NPT continues to strive towards making the project more impactful for CEs and hospital teams during a time where frontline clinicians and coordinating entities are more overextended than ever before. We are confident that the remaining two years of this project will yield powerful stories, meaningful data, and safer care for surgical patients. 13 | C U S P f o r S a f e S u r g e r y O p t i o n Y e a r O n e R e p o r t References 1. http://www.onthecuspstophai.org 2. Berenholtz SM, Lubomski LH, Weeks K, et al. Eliminating Central Line-Associated Bloodstream Infections: A National Patient Safety Imperative. Infect Control Hosp Epidemiol. (in press) 3. Wick EC, Hobson D, Bennett J, et al. Implementation of a Surgical Comprehensive Unit Based Safety Program (CUSP) to Reduce Surgical Site Infections. J Am Coll Surg 2012; 215(2): 193-200. 14 | C U S P f o r S a f e S u r g e r y O p t i o n Y e a r O n e R e p o r t Appendix A: Sample Ethnography Site Visit Memo 15 | C U S P f o r S a f e S u r g e r y O p t i o n Y e a r O n e R e p o r t 16 | C U S P f o r S a f e S u r g e r y O p t i o n Y e a r O n e R e p o r t 17 | C U S P f o r S a f e S u r g e r y O p t i o n Y e a r O n e R e p o r t 18 | C U S P f o r S a f e S u r g e r y O p t i o n Y e a r O n e R e p o r t