SPECIALTY PRIVILEGES
advertisement

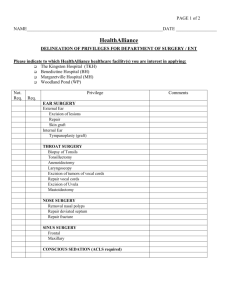
DEPARTMENT OF SURGERY DELINEATION OF PRIVILEGES FOR HAND SURGERY Name: ________________________________________________ Not Req. Req. Privilege Skin & Subcutaneous Tissues I & D of abscess Repair laceration superficial Repair laceration deep Fulguration skin lesions Excision and Repair Pinch/Davis Split Thickness Full Thickness Pedicle graft Rotation flap Treatment of Burns 1st degree 2nd degree 3rd degree Lymph Node I & D of Abscess Excision/Biopsy Musculo-Skeletal Repair of Muscle Repair of Tendon Repair of Nerve Excision of ganglions Release of nerves Elbow (Ulnar) Wrist (Median) Open Method Endoscopic Excision/biopsy of soft tissue Excision/biopsy of bones Total excision of tumors Amputations Finger Hand Forearm/arm Date: __________________ Disarticulation, shoulder Orthopedic Hand Removal of Foreign Bodies Percutaneous drainage of Abscess Hematoma Cyst Extremities - Plastic repair of Tendons/muscles Joints Fascia Nerves Bones (hand only) I have requested only those privileges for which by education, training, current experience and demonstrated performance I am qualified to perform. I also request the ability to do any procedure in an emergency situation. Applicant’s Signature: ________________________________________ Date: ________________ As part of the appointment / reappointment process, I, as Chairman of the Department, have reviewed this physician’s privileges and recommend approval or continuation of these privileges and the additions noted. Department Chair’s Signature: ___________________________________Date: ________________ Broadway and Mary’s Avenue Campuses