clinical considerations of lower limbs
advertisement

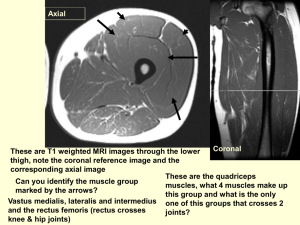
Clinical Considerations of lower limbs -Upon examination of a patient, it is found that the patient is unable to extend his/her knee against resistance. Further examination leads you to tap the patellar ligament with a percussion hammer to elicit the knee jerk reaction. However, there is no response. Q-What nerve could be damaged? What muscles are innervated by this nerve? A-Damage to the femoral nerve can cause impaired flexion of the hip (iliacus) and impaired extension of the leg due to paralysis of the quadriceps femoris. The patellar reflex is blocked by damage to the femoral nerve or a component of the patellar reflex arc. When normal the reflex arc should cause extension of the leg via the quadriceps muscle contraction. Q-An individual is stabbed in the popliteal fossa. Upon examination there is no damage to the major vessels in the area (popliteal artery and vein). However, the patient appears to have damage to the tibial nerve also found in the popliteal fossa. What possible functions are diminished or gone? A-The tibial nerve innervates the posterior compartment. The flexor compartment of the leg and intrinsic muscles of the foot would be affected. Thus, inversion and plantar flexion would be lost due to loss of innervation of the tibilialis anterior. The toes would be unable to be flexed due to loss of the flexor digitorum longus and flexor hallucis longus. The individual would have difficulty getting the heel off the ground without plantarflexing. - Venous return largely depends on muscular activity of the triceps surae which pump blood into the deep veins. When valves of the perforating limb become dilated they are unable to prevent reverse flow through veins and blood flows from deep to superficial veins. As a result, perforating and superficial veins become torturous and dilated and become varicose veins. Q-What are the main superficial veins in the leg and what deep veins do they drain into? Where are they usually located in the leg? A-The great saphenous vein ascends anterior to the medial malleolus of the tibia accompanied by the saphenous nerve and drains into the femoral vein by passing through the saphenous opening in the deep fascia of the thigh. The small (short) saphenous vein begins posterior to the lateral malleolus passing between the two heads of the gastrocnemius to enter the popliteal fascia to end in the popliteal vein. Q-What do people refer to when they speak of groin injuries? A-It refers to strain, stretching, and tearing away of the attachments of the anterior and medial muscles of the thigh. The attachments of these muscles are located in the inguinal region (junction of the abdomen and thigh) Q-You need to perform a left cardiac angiography and want to find the femoral artery when it is in a superficial location. Where could you palpate for the pulsations of the femoral artery? Where is the femoral vein in reference to the femoral artery? A-The superficial part of the femoral artery before it dives deep is in the femoral triangle. The femoral vein is found lateral to the artery. (i.e. NAVEL) The femoral artery and vein are found in the femoral sheath (Fig 5-32 Moore) Q-An individual walks with a waddling gait known as a gluteal gait. When the person lifts his/her right foot the pelvis falls on the left side. What could be happening? A-The gluteal gait is usually caused by paralysis of the gluteus medius muscle which is innervated by the superior gluteal nerve. This muscle usually functions to stabilize the pelvis when the opposite foot is off the ground. Q-When injecting drugs into the thigh. What nerves can be damaged and thus what regions should be avoided for intramuscular injections. A-Injections are performed in the anterolateral portion of the thigh. This avoids injury to the sciatic nerve which divide into the common fibular nerve and the tibial nerve. Also avoids injury to gluteal nerves. To avoid injury to the femoral nerve the injection should be done posterior to the anterior superior iliac spine. Thus what muscle(s) would you probably inject into to avoid both regions? (tensor fasciae lata and vastus lateralis) Q-Because the heads of the biceps femoris have a different nerve supply a wound in the thigh may sever a nerve paralyzing one head but not the other. What nerve supplies each head? A-Short head-Common fibular nerve Long Head-Tibial nerve Q-An individual comes in with laceration at the side of the knee and presents with loss of eversion of the foot and dorsiflexion of the foot. This results in foot drop where the foot is raised so toes do not hit the ground. There is also some loss of sensation in the anterolateral aspect of the leg and the dorsum of the foot. A-Laceration of the common fibular nerve results in loss of dorsiflexion of the foot since the anterior compartment of the leg is innervated by the deep peroneal nerve a branch of the common peroneal nerve. The lateral compartment containing the fibularis longus and brevis is innervated by the superficial peroneal nerve, the other branch of the common fibular nerve. See Case 5-2 Moore Causes for damage to the common fibular nerve can be deduced by its relations. Its relations to the biceps femoris tendon, the fibula, and the fibular collateral ligaments is important. Damage to any of these structures could cause damage to the adjacent common peroneal nerve. Q-What are the functions of the tibial and fibular collateral ligaments, how are they caused, and what are consequences of injuries to these structures? A-The two ligaments prevent disruption of the sides of the knee joint and prevent rotation of the tibia laterally and the femor medially. The fibular collateral ligament is very strong and not commonly torn. Severe blows to the MEDIAL side of the knee would force the knee towards the lateral side and tear the fibular collateral ligament. The tibial collateral ligament is attached to the medial meniscus and damage to this ligament can lead to damage to the medial meniscus as well. Damage is frequently caused by blows to the LATERAL side of the knee which would force the knee medially and tear the tibial collateral ligament. Q-Where are the ACL and PCL found. What purpose do they serve in the knee joint? How are they usually damaged? How can you test for damage to either of these ligaments of the knee joint? A-The ACL is the weaker of two ligaments and arises from the anterior part of the intercondylar area of the tibia to attach to the medial side of the lateral condyle of the femur. The anterior cruciate ligament prevents anterior dislocation of the tibia. The ACL injury is often associated with injuries to the medial meniscus and tibial collateral ligament. The ACL is damaged if the knee is severely hyperextended, tibia is driven anteriorly, or femur is driven posteriorly. To test the stability of the ACL one should test its function. Try to move the tibia anteriorly. If it moves a tear of the ACL is indicated. The PCL is the stronger of the two ligaments and arises from the posterior part of the intercondylar area and attaches to the lateral side of the medial condyle of the femur. The posterior cruciate ligament prevents posterior displacement of the tibia and hyperextension of the knee. The PCL is torn when the tibia is driven posteriorly on the femur when the knee is flexed (i.e. when knee hits dashboard in an accident) or if the knee is hyperflexed. To test the function of the posterior cruciate ligament test for its ability to prevent posterior displacement of the tibia. (See fig 5-108) In summary: Femoral nerve damage-impaired flexion of the hip and impaired extension of the leg due to paralysis of the quadriceps femoris Obturator nerve damage-impaired adduction and lateral swinging of the limb during walking because of unopposed abductors. Common fibular nerve damage-foot drop and paralysis of dorsiflexor (anterior compartment) and evertor muscles (lateral compartment) of the foot. Tibial nerve damage-Loss in plantar flexion, inversion of the foot, and flexion of the toes. (Posterior compartment of the leg) Deep peroneal nerve-loss of dorsiflexion Superficial peroneal nerve-loss of eversion Also look at the clinical problems in Moore.