Reducing Surgical Site Infections
advertisement

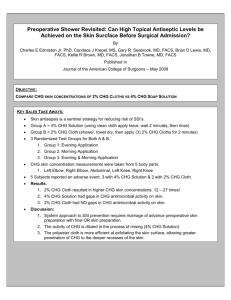
Reducing Surgical Site Infections Henry Rhee, MD and Bonnie Harris, CIC 03/01/2008 Disponible en http://www.infectioncontroltoday.com/articles/reducing-surgical-infections.html By definition, a surgical site infection (SSI) is an infection that develops within 30 days after an operation or within one year if an implant was placed and the infection appears to be related to the surgery. 1 Postoperative SSIs are the most common healthcare-associated infection in surgical patients, 1 occurring in up to 5 percent of surgical patients.2 In the United States, between 500,000 and 750,000 SSIs occur annually.3,4 Patients who develop an SSI require significantly more medical care. If an SSI occurs, a patient is 60 percent as likely to spend time in the ICU after surgery than is an uninfected surgical patient,5 and the development of an SSI increases the hospital length of stay by a median of two weeks. 6 The risk continues after discharge: SSIs develop in almost 2 percent of patients after discharge, 3 and these patients are two to five times as likely to be readmitted to the hospital. 5,6 The high morbidity and increased need for hospital care associated with SSIs contributes to increased healthcare costs. In a case-control study, patients with methicillin-resistant Staphylococcus aureus (MRSA) SSI had median hospital charges of $92,363, which was $62,908 more than the median charge for the control group of uninfected surgical patients.7 Mean attributable costs for SSI were $25,546 in a recent analysis of published studies on SSI costs.8 Other studies have estimated excess costs to range from $3,089 to a mean of $35,367 for MRSA infection.5,9 The increased cost is not confined to economic costs, because SSIs also contribute significantly to mortality. More than 20,000 deaths per year are due to SSIs,10 and the chance of death in a surgical patient is doubled if an SSI occurs.5 The increased mortality is even more pronounced after coronary bypass surgery, where deepchest SSI is associated with a mortality rate of 22 percent compared with 0.6 percent in those without an SSI. 11 The impact on hospitals of these additional costs will increase, because the Centers for Medicare and Medicaid Services (CMS) has adopted payment rules that go into effect in 2008 that will deny reimbursement for at least one SSI (mediastinitis from cardiac surgery). 12 Such moves reflect the general trend toward establishing improved standards of care, such as the 5 Million Lives initiative of the Institute for Healthcare Improvement (IHI) and the Surgical Care Improvement Project (SCIP), that seek to use education and intervention to reduce medical harm from SSI, infection with MRSA, and surgical complications. 13 Prevention of SSI requires addressing the causes. Although some of the risks are difficult to remedy, adequate skin antisepsis is a promising way to decrease rates of SSI, because contamination from bacteria at the surgical site is a necessary precursor to infection. 1,14 The Centers for Disease Control and Prevention (CDC) recommend the use of hand hygiene, skin antisepsis and surgical instrument and environment management (among other interventions) to reduce the risk of SSI. 1 Preoperative antisepsis should be done with an agent with a broad spectrum of activity and a rapid onset with persistent effects. The most commonly used skin antisepsis agents are iodine- and alcohol-based products and chlorhexidine gluconate (CHG). Alcohol-based products are effective, inexpensive, and readily available but are potentially flammable and can irritate the skin. CHG and iodine-based products both have a broad spectrum of activity, but CHG leads to greater reductions in skin microflora and offers greater residual activity. 1,15 In addition, CHG is not inactivated by blood or serum proteins as are iodine-based antiseptic products.1 The persistence of CHG on the skin allows prolonged and cumulative antibacterial effect. 16 The Food and Drug Administration (FDA) requires that antiseptics demonstrate a rapid 3.0 log10 reduction from baseline on a groin test site, a 2.0 log10 reduction on an abdomen test site and maintain effectiveness for at least six hours after application. 17 Recent research has shown that a 2 percent CHG impregnated alcohol-free no-rinse cloth for use for presurgical skin preparation is associated with excellent, rapid reductions of bacterial counts, with a minimum inhibitory concentration of 1:2,048 against Acine tobacter baumannii and >1:8,192 against MRSA and a 99.9 percent reduction from 15 seconds for A. baumannii and three minutes for MRSA.18 In addition, the 2 percent CHG no-rinse cloth appears to be more effective at reducing skin colonization than a 4 percent CHG solution that must be rinsed off.4 This may be the result of a residual effect and the gentle exfoliation caused by the no-rinse cloth. Although the need for skin antisepsis is well accepted, a few practical problems are associated with patient participation. The CDC recommends that patients shower or bathe with an antiseptic on at least the night before the operative day.1 Problems with having a patient shower or bathe include difficulty in determining whether the patient was compliant, patients who are unable to shower or bathe, and consistency in the method of preparation. To manage these potential problems and determine whether consistent, effective preoperative skin bathing works, staff at Prince William Hospital, a 170-bed acute care facility in Manassas, VA., developed an alternative preoperative bathing protocol. The protocol provided patients with a prepared, packaged bathing product and instructions on its use while the patient was in preoperative holding. Prince William Hospital participates in SCIP, and this study specifically sought to determine whether the hospital’s preexisting SSI rate of 2.1 percent could be reduced to the IHI/SCIP goal of 0 percent in surgery-bound patients. The current study is a pilot study that was initiated to evaluate the use of a preoperative patient preparation protocol with a prepackaged 2 percent CHG-impregnated no-rinse cloth (Sage® 2 percent CHG Cloth manufactured by Sage Products Inc.). The primary outcome measure was the rate of SSI with use of the 2 percent CHG no-rinse cloth compared with the background SSI rate. Methods The study was performed at Prince William Hospital. Patients were eligible for inclusion in the study if they were undergoing a surgical procedure. Approval for the study was obtained from the institution. Patients were asked for consent for inclusion in the study upon arrival in the preoperative area. The study was an observational pilot study that compared observed rates of SSI after institution of a 2 percent CHG no-rinse cloth preoperative preparation with historical rates of SSI at Prince William Hospital. The historical rates were based on an observation period from December 2005 through September 2006. The new preoperative protocol was instituted in August 2006 for same-day and outpatient surgery and in January 2007 for inpatient surgeries. The SSI rate associated with the new preoperative protocol was monitored from October 2006 through July 2007. Upon arrival at the hospital, patients were educated on the use of the CHG cloth by the operating room preoperative nurses with the use of an instruction sheet. The patients then washed themselves with the cloth as instructed. Nursing assistance was provided as needed if requested by the patient. The patients were instructed not to shave the operative site and were required to sign the instruction form to verify that they had read the instructions and had used the cloths according to the instructions. The cloths were supplied in prepackaged units; after January 2007, these were warmed before use to decrease the risk of hypothermia. The patients were instructed to allow the area to air-dry after prepping. The cloths were used to prep the entire body from the jawbone down to the toes. Each cloth was used for approximately 30 seconds and was disposed of after use. The patient was instructed to not apply lotion, moisturizers, or makeup. Upon completion of these steps, the patient signed the form and returned it to the nurse. Completed forms were then forwarded to the infection control department for review and data collection. The primary outcome measure was the rate of SSI with use of the 2 percent CHG no-rinse cloth protocol. A secondary outcome measure was compliance with the protocol (the number of patients completing the instructions). The primary and secondary outcome measures were reported as actual numbers and percentages and were compared with the historical rates. Because this was an observational pilot study, no further statistical analysis was done. Results During the 10 months before institution of the protocol (the historical observation period), a total of 5,174 procedures was done. During the 10 months after institution of the protocol (the observational pilot study period), 4,266 procedures were done. Primary Outcome Data There was a total of 25 SSIs during the historical observation period and 11 SSIs during the pilot study period. During the historical observation period, 18 patients required readmission; during the pilot study period, only five patients required readmission. The average SSI rate was 2.1 percent during the historical observation period and was 0.7 percent during the pilot study period. This represents a 66 percent difference in the rate of infections for monitored procedures and a 72 percent difference in the rate of readmission due to SSI. Secondary Outcome Data The average cost due to SSIs was $648,471 before the intervention and $290,827 after the intervention. The investment costs for the product were $8,721, leaving a cost savings of $348,923 (pre-intervention cost minus post-intervention cost plus product costs). Pre-intervention readmission costs were $221,075, and postintervention readmission costs were $43,000, reflecting a cost savings of $177,937. One patient developed an allergic reaction and was treated with diphenhydramine for itching, and a second patient experienced a minimal rash. Another patient refused the product because of concern about a potential allergy. No serious adverse events occurred. Discussion Previous studies showed that CHG is effective in reducing bacterial counts on the skin. Kaiser et al., found that CHG was more effective than povidone-iodine in reducing skin colonization with staphylococci and that repeated applications of CHG were superior to a single shower. 15 A fullbody 4 percent CHG shower reduces bacterial counts at abdominal and inguinal sites,16 and a 4 percent CHG two-minute surgical scrub has been shown to reduce microbial counts better than povidone-iodine.19 Recent data from DeBaun confirms a 99.9 percent reduction in MRSA after three minutes of exposure to CHG and Acinetobacter after 15 seconds of exposure. 18 These studies show the effectiveness of CHG in reducing bacterial counts, which may, in turn, reduce SSI rates. Given today’s healthcare environment and patient concerns with MRSA, which they refer to as ‘superbugs,’ it seems prudent to have patients apply full-skin antisepsis before entering the operating room. Although it would be expected that skin antisepsis would reduce SSI rates, studies of previously available skin antiseptics yielded mixed results. A Cochrane review of preoperative showering or bathing with 4 percent CHG did not demonstrate significant benefit over other products, including regular soap.20 In a second Cochrane review of preoperative skin antiseptics, the author concluded that there was too much heterogeneity between studies of antiseptic products to pool the results. 21 CHG solution reduced SSIs compared with iodine-based products in one study, whereas four studies of iodinebased preps found no reduction in SSIs. 21 These studies examined the benefits of using a 4 percent CHG solution, however, and it appears that a 2 percent CHGimpregnated cloth may be more effective for preoperative skin antisepsis. Edmiston, et al., found that although both 4 percent CHG solution and a 2 percent CHGimpregnated cloth were effective at reducing bacterial counts, the application of CHG with the 2 percent cloth led to greater reductions in microbial counts than the 4 percent CHG solution.4,22 This may be a result of the gentle exfoliation associated with the use of the cloth.4 It is also possible that the cloth leaves more CHG residual, because the product does not require rinsing after use. In the current pilot study, the 2 percent no-rinse cloths reduced the rate of SSI compared with a historical observation period. When a full 10 months of data are used for the historical rate and 10 months of data are used for the protocol SSI percentage rate, the rate of SSI drops by 66 percent. Addition of the 2 percent CHG no-rinse cloth protocol ensured documented patient compliance as opposed to undocumented showering with chlorhexidine at home. In addition, the norinse nature of the CHG cloth may result in greater CHG residual on the skin. It is also possible that the exfoliative nature of the product improves its performance. Last, in previous studies, it was shown that reducing hypothermia can reduce SSIs.23 Thus, by warming the cloths before use, it is possible that the likelihood of hypothermia associated with bathing was decreased. The strengths of this study were its prospective nature and that a large number of procedures were monitored. Because this was a pilot study and not a controlled study, further analysis of results and direct comparison with another product was not done. Also, the lack of a control group prevented estimation of the relative benefits of avoiding hypothermia in the study group. Conclusion SSIs are a serious medical problem associated with increased morbidity and mortality and increased medical care costs. This study showed that a new presurgical preparation protocol using warmed 2 percent CHGimpregnated no-rinse cloths led to reduced rates of SSI compared with a historical observation period. This reduction in SSIs, in turn, led to reduced medical costs, even when the cost of the 2 percent CHG no-rinse cloths was taken into account. Self-application of pre-warmed 2 percent CHG cloths contributed to patient comfort and satisfaction, possibly contributing to improved compliance. Because of these promising results, our facility has chosen to continue to use the 2 percent CHG no-rinse cloths for all surgical procedures. References 1. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR, the Hospital Infection Control Practices Advisory Committee. Guideline for the prevention of surgical site infection, 1999. Infect Control Hosp Epidemiol. 1999;20:247-280. 2. Cheadle W G. Risk factors for surgical site infection. Surg Infect. 2006;7 Suppl 1:S7-11. 3. Perencevich EN, Sands KE, Cosgrove SE, et al. Health and economic impact of surgical site infections diagnosed after hospital discharge. Emerg Infect Dis. February 2003;9(2):196-203. 4. Edmiston CE, Seabrook GR, Johnson CP, Paulson DS, Beausoleil CM. Comparative of a new and innovative 2 percent chlorhexidine gluconate-impregnated cloth with 4 percent chlorhexidine gluconate as topical antiseptic for preparation of the skin prior to surgery. Am J Infect Control. 2006; 35(2):89-96. 5. Kirkland KB, Briggs JP, Trivette SL, et al. The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect Control Hosp Epidemiol. 1999;20:725-730. 6. Whitehouse JD, Friedman D, Kirkland KB, Richardson WJ, Sexton D. The impact of surgical site infections following orthopedic surgery at a community hospital and a university hospital: adverse quality of life, excess length of stay, and extra cost. Infect Control Hosp Epidemiol. 2002;23(4): 183-189. 7. Engemann JJ, Carmeli Y, Cosgrove SE, et al. Adverse clinical and economic outcomes attributable to methicillin resistance among patients with Staphylococcus aureus surgical site infection. Clin Infect Dis. 2003;36(5):592-598. 8. Stone PW, Braccia D, Larson E. Systematic review of economic analyses of health care-associated infections. Am. J. Infec. Control. 2005;33(9):501-509. 3 ICT www.infectioncontroltoday.com March 2008 9. Stone PW, Larson E, Kawar LN. A systematic audit of economic evidence linking nosocomial infections and infection control interventions: 1990-2000. Am J Infect Control. 2002;30:145-152. 10. Woods A. Key points of the CDC’s Surgical Site Infection Guideline. Adv Skin Wound Care. 2005;18(4):215220. 11. Hollenbeak CS, Murphy DM, Koenig S, et al. The clinical and economic impact of deep chest surgical site infections following coronary artery bypass graft surgery. Chest. August 2000;118(2):397-402. 12. Centers for Medicare and Medicaid Services. Available at: http://www.cms.hhs.gov/apps/media/press/factsheet.asp?Counter=2119&intNumPerPage=10&checkDate=&che ckKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=6&intPage=&s howAll=&pYear=&year=& desc=&cboOrder=date Accessed Oct. 1, 2007. 13. Institute for Healthcare Improvement 5 Million Lives Campaign. Available at: http://www.ihi.org/IHI/Programs/Campaign/Campaign.htm?TabId=1 Accessed Oct. 9, 2007. 14. Pottinger JM, Starks SE, Steelman VM. Skin Preparation. Perioperative Nurs Clin. 2006;1:203-210. 15. Kaiser AB, Kernodle DS, Barg NL, Petracek MR. Influence of preoperative showers on staphylococcal skin colonization: a comparative trial of antiseptic skin cleansers. Ann Thorac Surg. 1988;45(1):35-38. 16. Paulson DS. Efficacy evaluation of a 4 percent chlorhexidine gluconate as a full-body shower wash. Am J Infect Control. 1993;21(4):205-209. 17. Food and Drug Administration, 21CFR Parts 333 and 369. Tentative final monograph for healthcare antiseptic drug products: proposed rules. Federal Register Part III, 1994;59(116): 31401-31452. 18. DeBaun B. New Alcohol-Free 2 percent CHG Solution Reduced Bacterial Counts of Drug-Resistant Acinetobacter and MRSA by 99.9 percent. Poster presented at the 2007 Association of periOperative Registered Nurses (AORN) Congress, Orlando, Fla. Mar 2007. 19. Aly R, Maibach HI. Comparative antibacterial efficacy of a 2-minute surgical scrub with chlorhexidine gluconate, povidoneiodine, and chloroxylenol sponge-brushes. Am J Infect Control. 1988;16(4):173-177. 20. Webster J, Osborne S. Preoperative bathing or showering with skin antiseptics to prevent surgical site infection. Cochrane Database Syst Rev. 2007;(2):CD004985. 21. Edwards PS, Lipp A, Holmes A. Preoperative skin antiseptics for preventing surgical wound infections after clean surgery. Cochrane Database Syst Rev. 2004;(3):CD003949. 22. Edmiston C, Seabrook GR, Johnson CP, et al. Comparison of a New and Innovative 2 percent Chlorhexidine Gluconate (CHG) Impregnated Preparation Cloth with the Standard 4 percent CHG Surgical Skin Preparation. Poster presented at the 2007 Association of periOperative Registered Nurses (AORN) Congress, Orlando, Fla. Mar 2007. 23. Kurz A, Sessler DI, Lenhardt R. Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalization. Study of Wound Infection and Temperature Group. N Engl J Med. 1996 May 9;334(19): 209-1215.