Respiration-3
advertisement

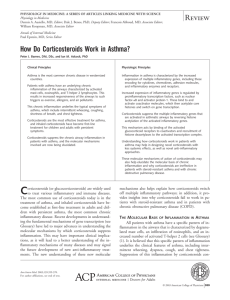
DRUGS USED IN THE TREATMENT OF ASTHMA - ANTI-INFLAMMATORY AGENTS Dr Stuart Wilson DRUGS USED IN THE TREATMENT OF ASTHMA - ANTI-INFLAMMATORY AGENTS CORTICOSTEROIDS Adrenal cortex synthesises two major classes of steroid hormone that are released into the circulation. Not pre-stored, but synthesised and released on demand. Glucocorticoids – the main hormone is cortisol (hydrocortisone) regulates numerous processes that are essential to life, e.g: carbohydrate and protein metabolism Hypothalamus responses to stress inflammatory responses Synthesis and release of cortisol Cortisol regulated by adrenocorticotrophic hormone (ACTH) released from the anterior pituitary. Release of ACTH is partially under negative feedback control by the level of cortisol in the blood (see Endocrinology block) Pituitary ACTH + Adrenal cortex Mineralocorticoids – mainly aldosterone - regulates the retention of salt (and water) by the kidney Synthesis and release of aldosterone are regulated mainly by the renin-angiotensin system (see Cardiovascular and Renal blocks) Naturally occurring steroids may possess both glucocorticoid and mineralocorticoid actions. The latter are unwanted in treatment of inflammatory conditions Synthetic derivatives of cortisol, that have little, or no, mineralocorticoid activity are frequently used for their antiinflammatory effect in the treatment of asthma and many other conditions. They have no direct bronchodilator action and are ineffective in relieving bronchospasm when given acutely MOLECULAR MECHANISM OF ACTION OF STEROID HORMONES Steroid hormones are lipophilic molecules - enter cells by diffusion across the plasma membrane (1) 1 2 3 Nucleus 4 Transcription (5) mRNA (6) Translation (7) Proteins (8) Within the cell, they combine with an intracellular receptor (2) producing a conformational change exposing a DNA-binding domain (3). In the case of the glucocorticoids, the inactive receptor is located in the cytoplasm The receptor steroid complex moves to the nucleus (4) and binds to steroid response elements in DNA The transcription of specific genes (5) is either ‘switched-on’ (induced) or ‘switched off’ (repressed) to alter mRNA levels (6) and the rate of synthesis (7) of mediator proteins (8) GLUCOCORTICOID EFFECTS UPON GENE TRANSCRIPTION THAT ARE RELEVANT TO INFLAMMATION IN BRONCHIAL ASTHMA Many tens of genes are regulated by glucocorticoids acting at GREs, or by modifying chromatin (via deacetylation of histones – not discussed here) Gene activation (generally high doses of glucocorticoids) Examples: Annexin-1 (lipocortin-1) -adrenoceptors IB- (inhibitor of the inflammatory transcription factor NF-B) Gene repression (occurs with low doses of glucocorticoids) Examples: Cytokines Chemokines Adhesion molecules Inflammatory enzymes Inflammatory receptors GLUCOCORTICOID EFFECTS UPON GENE TRANSCRIPTION THAT ARE RELEVANT TO INFLAMMATION IN BRONCHIAL ASTHMA (Example 1) Gene induction Increased synthesis of annexin-1 (lipocortin-1), a polypeptide inhibiting the enzyme phospholipase A2, decreases the formation of leukotriene spasmogens (LTC4, LTD4) and chemotaxins (LTB4) by reducing the formation of precursor arachidonic acid. Membrane phospholipid X Phospholipase A2 Arachidonic acid Lipocortin-1 blocks 5-lipoxygenase LTB4 (chemotaxin) Infiltration of eosinophils LTA4 LTC4 & LTD4 CysLT receptor activation and bronchoconstriction GLUCOCORTICOID EFFECTS UPON GENE TRANSCRIPTION THAT ARE RELEVANT TO INFLAMMATION IN BRONCHIAL ASTHMA (Example 2) Gene repression Decreased formation of protein cytokines that: 1) recruit and activate eosinophils and 2) promote the production of IgE and expression of IgE receptors Glucocorticoids block Th2 X B P IgE B P IgE Cytokines B CELLULAR EFFECTS OF GLUCOCORTICOIDS RELEVANT TO ASTHMA From Barnes, P.J. (2006). Eur. J. Pharmacol. 533, 2-14. CLINICAL USE OF GLUCOCORTICOIDS IN ASTHMA Glucocorticoids suppress the inflammatory component of asthma – (1) prevent inflammation and (2) resolve established inflammation Short term, they do not alleviate early stage bronchospasm caused by allergens, or exercise, but long term treatment is effective very effective (particularly in combination with a long-acting 2-adrenoceptor agonist) In mild/moderate asthma: Glucocorticoids (often beclomethasone) are given by inhalation from a metered dose inhaler (to minimise many unwanted systemic effects) Efficacy develops over several days The most common adverse effects (due to deposition of steroid in the oropharynx) are: 1) dysphonia (hoarse and weak voice) 2) oropharyngeal candidiasis (thrush) In chronic, severe, or rapidly deteriorating asthma Oral prednisolone may be used in combination with an inhaled steroid to reduce the oral dose required and minimise unwanted systemic effects. Bronchodilator drugs are co-administered (See lectures by Prof. Lipworth for greater clinical detail) CROMOGLYCATES Are second line drugs used prophylactically in the treatment of asthma (particularly children) Have no direct effect upon bronchial smooth muscle Have an uncertain molecular mechanism of action. A decrease in the sensitivity of irritant receptors associated with sensory Cfibres that trigger exaggerated reflexes and reduction of cytokine release are potential mechanisms SPECIFIC AGENT Sodium cromoglycate delivered by inhalation can reduce both phases of an asthma attack, but efficacy may take several weeks to develop Is the anti-inflammatory of choice in some children RECENT APPROACHES TO THE TREATMENT OF ASTHMA THAT INVOLVE ANTI-INFLAMMATORY ACTIONS Monoclonal antibodies directed against IgE (e.g. omalizumab) • Binds IgE via Fc to prevent attachment to Fc receptors – suppresses mast cell response to allergens • Reduces the expression of Fc receptors on various inflammatory cells From Strunck, R.C. and Bloomberg, G.R. (2006) N. Engl. J. Med. 354, 2689-2695.