Prenatal screening for genetic
disorders: best current practice and
what’s around the corner
June C Carroll MD CCFP FCFP
Sydney G Frankfort Chair in FM
Associate Professor and Research Scientist
Department of Family & Community Medicine
Mount Sinai Hospital, University of Toronto
OCFP 51st ASA, November 29, 2013
Objectives
• Prenatal screening for genetic disorders
―FTS/IPS/MSS
―Non-invasive prenatal testing (NIPT)
―Use of microarray for prenatal diagnosis
• Ethnicity based screening
• Consanguinity and genetics
Prenatal Screening tests for:
DS, T18, T13 and ONTD
Factors affecting FTS/IPS screening
performance…and why you need to record
them on the requisition
• Gestational dating
―FPR lowered by ~2% when GA estimated using scan
• Maternal weight
―Negative association between levels of maternal serum
markers and maternal weight due to dilution effect
produced by increased blood volume
―Weight adjustment
• increases DR by ~1% for a given FPR
• reduces FPR by 0.2% for given DR
• Ethnic origin
―Adjusting tends to equalize the FPR among women of
different ethnic groups
SOGC Guidelines 2011
Factors affecting FTS/IPS screening
performance…and why you need to record
them on the requisition
• Insulin-dependent diabetes mellitus
―Some T2 markers are lower
• Smoking
―Affects risk calculations – indicate if any smoking during
pregnancy (even at time of conception)
• Assisted Reproduction
―Maternal age used is age of donor or woman at time egg
was harvested
―IVF pregnancies have higher risk of false positive screen –
correction factor used – so important to indicate
SOGC Guidelines 2011
Prenatal Genetic Screening
• Maternal age
―Practice of using solely maternal age at EDD to
identify at-risk pregnancies should be abandoned
• DR for DS: 44%, FPR 16%
―Maternal age should not be used as a basis for
recommending invasive testing when non-invasive
PN screening is available
―Modify age-related risk by multiple biochemical
markers with or without first trimester u/s
assessment of nuchal translucency
SOGC Guidelines 2011
Use of Ultrasound in Screening for
Chromosomal Anomalies
• Detailed u/s at 18-20 weeks’ gestation
• Most major fetal anatomic abnormalities will be
detected
―Majority of ONTD
• Soft markers
―Should not be used alone
―Use to modify any a priori risk established by age or prior
screening
―In absence of soft markers and anomalies – reduction of
risk of 0.5 can be applied – only in tertiary level scan
centre
―See 2007 SOGC Ultrasound Soft Marker Guideline
SOGC Guidelines 2011
Prenatal Screening with addition of
Non-invasive Prenatal Testing (NIPT)
•
•
•
•
What is NIPT?
What is the evidence for NIPT?
What do the experts say?
What is current Ontario prenatal screening
landscape?
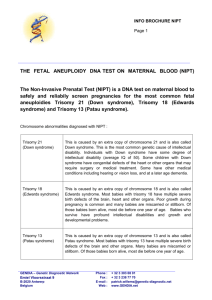
What is Non-invasive Prenatal Testing
(NIPT)?
• Screening test to prenatally detect Down
syndrome and other aneuploidies (extra or
missing chromosomes)
― trisomy 21, 18, 13
― trisomy of sex chromosomes (XXX, XXY, XYY)
― Turner syndrome (monosomy X)
― triploidy (extra copy of all chromosomes)
NIPT
• NIPT measures circulating cell free fetal DNA (ccffDNA)
present in maternal blood (from trophoblast)
• Comprises ~10% of DNA in maternal blood
• Increases with gestational age
• ccffDNA analysis determines if normal, higher, or lower
than expected quantity of particular DNA sequences
found on select chromosomes (13, 18, 21, X, Y)
• Performed on maternal blood sample
• As early as 9 weeks’ gestation
• Dating u/s – viability, accurate GA, exclude multiples
What’s the evidence for NIPT?
• 7 studies of “high risk” women
• High risk:
―Screen positive
―AMA (≥35 yrs)
―Ultrasound findings
―Family history indicating increased risk
• Previous pregnancy with aneuploidy
What’s the evidence for NIPT?
• By far most accurate performance for T21/18
Benn et al, Ultras Obstet Gynecol 2013, 42: 15-33
What’s the evidence for NIPT?
• 4 studies on unselected pregnancies
―Most mixed risk, some after pos screen, AMA,
fewer with neg or no screen
―> 14,000 pregnancies total, largest (11,000
significant loss to follow up)
―Similar performance
• Not yet validated in low risk women, triplets or
higher, pregnancies conceived with egg
donation
Benn et al, Ultras Obstet Gynceol 2013, 42: 15-33
What’s the evidence for NIPT?
• Failed results
―6.1% (0.8-9.9) untested for insufficient sample
quality
―2% (436/22,222) no result after testing
―Rarely happens with conventional screening
―ccffDNA decreases with increased maternal BMI
Benn et al, Ultras Obstet Gynceol 2013, 42: 15-33
Summary of evidence for NIPT
Disorder
Sensitivity
FPR
Down syndrome
99-100%
~0.1%
Trisomy 18
97-100%
~0.1%
Trisomy 13
79-92%
~0.1%
Sex chromosome
differences
94-99%
Benn et al, Ultras Obstet Gynceol 2013, 42: 15-33
What do the experts say?
• American College of Obstetricians and
Gynecologists 2012
―Has been validated in industry sponsored studies
on at risk populations
• History of prior pregnancy with trisomy
• Positive multiple marker test
• Parental balanced Robertsonian translocation with
increased risk of fetal trisomy 13/21
• Maternal age >35
• Fetal ultrasound findings with increased risk of
aneuploidy
ACOG Committee Opinion: Dec 2012
What do the experts say?
• Society of Obstetricians & Gynecologists of
Canada 2013
Non-invasive
prenatal testing using massive
parallel sequencing of cell-free fetal DNA to test
for trisomies 21, 18, and 13 should be an option
available to women at increased risk in lieu of
amniocentesis. Pretest counselling of these
women should include a discussion of the
limitations of non-invasive prenatal testing.
Genetics Ctte Technical Update JOGC: Feb 2013
What do the experts say?
• Society of Obstetricians & Gynecologists of
Canada 2013
No irrevocable obstetrical decision should be
made in pregnancies with a positive non-invasive
prenatal testing result without confirmatory
invasive diagnostic testing.
Genetics Ctte Technical Update JOGC: Feb 2013
Recommendation in Ontario
• Offer all women prenatal screening using either FTS,
IPS or MSS (SIPS or Quad)
• IF screen +ve or at high risk for other reasons
―Consider NIPT as secondary screen of higher sensitivity if
she is willing to pay for the test
• High risk:
―Advanced maternal age
―Previous aneuploidy pregnancy
―Personal hx of sex chromosome aneuploidy (Turner
mosaic, XXX)
―Abnormal u/s
―Pregnancy conceived via reproductive technologies
Recommendation in Ontario
• NIPT is not a replacement for diagnostic PN
testing
• Positive NIPT should be confirmed by
diagnostic testing: amnio or CVS
• Expected benefit of NIPT: fewer women
having diagnostic tests with associated risk of
pregnancy loss
Recommendation in Ontario
• If result is negative → reassuring
• NIPT cannot:
―Completely rule out aneuploidy
―Detect chromosome differences other than
aneuploidy of chromosomes 13, 18, 21, X and Y
―Detect single gene conditions
―Detect congenital anomalies
• Still offer MSAFP and 18-20 wk ultrasound
Recommendation in Ontario
• If result is positive:
―Genetic counselling
―Confirmation by diagnostic testing
No irrevocable obstetrical decisions should be
made in pregnancies with abnormal NIPT
results without confirmatory invasive testing
(CVS or amnio) - SOGC
NIPT in Ontario
•
•
•
•
•
Increasing demand from women (who can pay)
Increasing uptake in most (urban) centres
3 separate companies, 3 separate technologies
No mechanism to evaluate centrally
Has it become mainstream now, become a
“standard of care”? (? Only for high risk women)
• Heading for 2 tiered prenatal screening
• Costs between $795 and $1200
• 8-10 days for result
Where does NIPT fit with respect to the
11 to 14 wk scan?
• 11 to 14 week scan has value to pregnancy care
―NT may shift in importance (importance to other
chromosomal, genetic and structural disorders)
―Accurate dating/establishment of live fetus
―Multiples/chorionicity affects management
―Detects structural abnormalities
NIPT and counselling
• Likely primary providers will not have
time/expertise to counsel in detail
• Refer to genetic counselling if your centre
provides that service (significant impact on
counselling demands)
• Company websites:
―Panorama™ by Lifelabs
―Harmony™ by Ariosa
―Verifi™ by Verinata Health (Medcan)
NIPT vs microarray: 2 diverging
philosophies
Chromosomal Microarray (CMA)
•
CMA is a technology used to determine if there are small extra (microduplication)
or missing (microdeletion) pieces of genetic information. These gains and losses
are called copy number variants (CNVs). A CNV can be: of no medical
consequence; pathogenic resulting in physical and/or intellectual consequences;
or protective against disease (e.g. HIV infection).
Reference DNA from control
labeled Red
Test DNA from patient
labeled Green
Denature the DNA (separate the strands) and Hybridize to slide
Areas of loss (deletion)
Glass microarray slide
Computer scans and
analyzes signal outputs
Area of gain (duplication)
Microarray for Prenatal Diagnosis
• Microarray can detect submicroscopic copy number
changes that are associated with clinically significant
outcomes
• Systematic review to calculate utility of PN microarray
in presence of normal conventional karyotype
―12,362 pregnancies
• 2.4% overall had copy number changes with associated
clinical significance
• 6.5% if ascertained because of abnormal ultrasound
• 1.0% if increased maternal age
• 1.1% for other reasons (parental anxiety, abnormal MSS)
Wapner NEJM 2012, Callaway Prenatal Dx 2013
Microarray for PN diagnosis
• Microarray generally detects all aneuploides
and unbalanced translocations identified on
karyotyping
―Does not identify balanced translocations/triploidy
Wapner NEJM 2012
Microarray for PN diagnosis
• Summary
―Consider when doing invasive test like CVS or amnio
―Added diagnostic value of microarray especially when
karyotype gives normal chromosome result
―Genetic consult will assist with which test is most appropriate
depending on clinical presentation
• karyotype, microarray or both
―Challenges:
• Variants of unknown significance
• Incidental findings
―Future:
• Next generation sequencing, whole genome sequencing
Wapner NEJM 2012, Callaway Prenatal Dx 2013
Ethnicity based screening
Ethnic Group
Black
Disorder
Screening test
Sickle cell anemia
MCV<80% followed by Hb
electrophoresis
DNA analysis
Ashkenazi Jewish
8 disorders
French Canadian
Tay-Sachs disease
Mediterranean
β-thalassemia
SE Asian
α-thalassemia
DNA analysis for selected
alleles
MCV<80% followed by HB
electrophoresis (r/o iron def)
MCV<80% followed by Hb
electrophoresis
Ethnicity based screening: Carrier testing for
persons of Ashkenazi Jewish background
Disease
Carrier frequency in AJ
Population
Bloom Syndrome
1/102
Canavan Disease
1/57
Familial Dysautonomia
1/32
Fanconi Anemia group C
1/89
Mucolipidosis IV
1/100
Niemann Pick (A&B)
1/90
Tay-Sachs Disease
1/30
Ethnicity based screening: Carrier testing for
persons of French Canadian background
- Charlevoix/Saguenay-Lac-Saint-Jean area
Disease
Carrier frequency
Cystic Fibrosis
1/15
Tyrosinemia type 1
1/21
Spastic Ataxia of Charlevoix-Saguenay
1/22
Hereditary Sensory-Motor Polyneuropathy
+/- Agenesis of Corpus Callosum
1/23
Cytochrome Oxidase Deficiency
1/23
Screen all Fr Can/Cajun descent for TSD – take a FH/ refer from regions above
Consanguinity
• Deeply rooted cultural trend among 1/5 of world
population
―Mostly residing in Middle East, West Asia, North Africa and
emigrants from these communities
―Intra-familial unions account for 20-15+% of all marriages
―First cousins 1/3 of all marriages
• Def’n: union between 2 people who are related as
second cousins (5th degree relatives) or closer
―First cousins, first cousins once removed, second cousins
Hamamy J Community Genetics 2012
Consanguinity
• Mainly cultural reasons for consanguineous
marriages
―Strategy to preserve transmission of cultural
values and continuity
―Maintenance of familial structure and property
―Financial advantage relating to dowry, keeping
property within family
―Sometimes thought to be more stable unions
• Same social relationships before and after marriage
Consanguinity
• Genetic Risk: first cousin marriages compared to
non-consanguineous marriages
―Fertility rate slightly higher
―Miscarriage rate not different
―Stillbirths and infant mortality rates slightly higher
―Congenital anomalies 2-3% higher than background
population risk (2-3%)
―Increased likelihood of autosomal recessive conditions
―Increased risk for almost all multifactorial birth defects
including congenital heart defects, clefting, club feet, etc
―Complex diseases – really not known – could be significant
if high susceptibility gene present in family
Hamamy J Community Genet 2012
Consanguinity
• Management
―Premarital/preconception counselling
• For carrier status
• May change marriage plans
―3 to 4 generation FH
―Appropriate testing based on FH and ethnic
background
• i.e. screen for common autosomal recessive conditions in
pop and community
―Refer to genetics if FH points to presence of genetic
disorder
Consanguinity
• Concerns
―Fear of stigmatization
―Belief that inherited disorders can only arise through
cousin marriages on paternal side – specifically
inquire re shared biologic relationships on mother’s
side
―Need to balance risks and benefits
Prenatal Screening Summary
• Offer all pregnant women, regardless of age, PN
screening for fetal aneuploidy (trisomy 13, 18, 21)
through FTS, IPS, SIPS or Quad screening
• + second trimester ultrasound for dating, assessment
of fetal anatomy and detection of multiples
• Maternal age should not be used as a basis for
recommending invasive testing when non-invasive
PN screening is available
• Consider offering NIPT to high risk women or
following a positive PN screen for aneuploidy
Prenatal Screening Summary
• Take a FH to identify familial and/or ethnically
related disorders and screen accordingly
• Consider consanguinity and screen and test
accordingly
• Refer or consult genetics when in doubt
Useful Genetics Resources
• GEC-KO website: Genetics Education Website
• www.gecko-cegco.ca
• NIPT fact sheets:
―http://www.mountsinai.on.ca/care/pdmg/NIPT%20info%20sh
eet%20for%20parents%2029_11_2012.pdf
―http://www.mountsinai.on.ca/care/pdmg/NIPT%20info%20sh
eet%20for%20For%20Healthcare%20Providers%2029_11_201
2.pdf
• Prenatal Screening Ontario Website
―http://www.prenatalscreeningontario.ca/
• morrison@cheo.on.ca, jcarroll@mtsinai.on.ca
• Thanks to Shawna Morrison, GEC-KO program manager for
assistance with this presentation