Sex differentiation
What makes us Male or Female?
Chromosomic Sex
•
karyotype
•
Chromosomic Sex
• Y Chromossome – SRY Gene – codes
for the testis determining factor.
In the absence of SRY there iare no
testes.
• X Chromossome – DSS – Double dose
gene. Two DSS genes are required for
the ovaries to be fully functional
Chromosomic number
Full trisomy of an individual occurs when a chromosome fails to saparate
during gamete formation. This can result in an extra or missing
chromosome in a sperm or egg cell. After fertilization, the resulting
fetus has 47/45 chromosome instead of the typical 46.
Partial/mosaic
• A partial trisomy occurs when part of an extra chromosome is
attached to one of the other chromosomes, or if one of the
chromosomes has two copies of part of its chromosome.
• A mosaic trisomy is a condition where extra chromosomal material
exists in only some of the organism's cells.
Sex chromosomes are special
• You cannot have any monosomy of any
chromosome other than X and Y. (in those
cases you can function just fine)
• Trisomies of sex chromosomes will be
expressed mostly in the reproductive area;
but not necessarily.
Bipotential Gonads
• In the presence of SRY – Testes
• In the absence of SRY – Ovary like
• Two doses of DSS needed to develop fully
functioning ovaries.
Brain
• Presence of androgens – Brain – Male
• Absence of androgens - Brain – Female
Genital Sex
Genital Sex
Brain Differentiation
• In the presence of SRY – Testes
• In the absence of SRY – Ovary like
• Two doses of DSS needed to develop fully
functioning ovaries.
Brain Lateralization
corpus
callosum
Size of the Anterior Commissure
in the Brain
It is a fiber tract that is larger in its midsagittal area in women
than in man
Brain – Sexual chemistry
Brain Differentiation Rats
Gender differentiation brain
What Makes Us Male or Female?
•
•
•
•
Chromosomic Sex
Gonadal Sex
Genital Sex
Brain Differentiation
Hand
Finger length correlates with the concentration of androgens in uthero
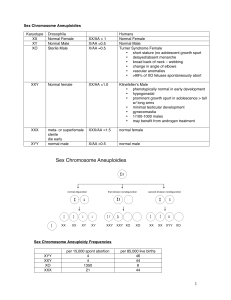
Chromosomic defects
XO – Turner
XXY - Klinefelter
Turner
Missing X Chromosome
Low hair line
Klinefelter syndrome
Extra X/Y Chromosome
Androgenized Genetic
Female Child
Genetic Female:XX
External Genitalia exposed to Androgens during genital
differentiation
Androgenized Genetic
Female Child
• Progestin Induced Virilization –
androgens given to mothers to prevent
miscarriages.
• Congenital Adrenal Hyperplasia – need
medical attention at birth.
• Some anticonvulsant drugs
• Pollutants?
Gender role preference behaviors in
congenital adrenal hyperplasia patients
Androgen
Insensitivity Syndrome
5-alpha reductase deficiency
• 5 alpha reductase deficiency is one of several conditions
where girls are bornwith XY genes (the usual male
pattern). It is not known how common 5 alphareductase
deficiency is, but it can run in families or it can be a
chance event.
• 5 alpha reductase deficiency is one of several conditions
where girls are born with XY genes (the usual male
pattern). It is not known how common 5 alpha reductase
deficiency is, but it can run in families or it can be a
chance event.
• External genitalia female – testes present. Secondary Sex
differentiation can include the growth of the clitoris
(virilisation) and descending of the tests hirsutism.
• In some parts of the world some girls born with this
condition have changed to start living as a boy and man
after puberty, but this is uncommon in Western Cultures.
Intersex
• True hermaphrodites: have both gonads
• Pseudo hermaphrodites: external genitalia
does not mach internal gonodal sex.
Gender Identity
• How a person perceives him/herself as male
or female
• Feeling of Maleness/femaleness or an
ambivalence between the two.
Gender Identity disorder
• Your concept of oneself (Male / Female)
does not mach genitalia
• Brain differentiation form of gender
intersex?
"When you work with these kids, you
see that they're not making a
decision," he says. "They have always
known. The sense of who one is--[boy
or girl]--is a crucial existential aspect
of humanity. It is powerful and
inborn." The absence or presence of a
penis is incidental. "The most
important sex organ is the brain."
Hopkins's William Reiner
Gender Dysphoria/Transsexualism
• Gender differentiation of the Brain occurs on the 3rd Trimester of
pregnancy.
• Characterized by strong disgust for the body and deep
uncertainty over the sense of self.
• Gender identity (the sense of either being male or female) is not
directly determined by the genetic code.
• congenital intersex condition, in which the genitalia are spared
prenatally but the brain is not.
• Transsexual persons ordinarily do not have a mental illness.
• A 1996 German study following 1422 gender-reassigned
transsexual GID patients over a ten-year period found that less
than 0.1% (1 in 1422) evidenced regret.
• Standards of Care now calls triadic treatment (surgery,
hormones and cross-living) medically indicated, medically
necessary, and proven effective, in profound GID or
transsexuality.
In the 60’s
•
•
•
•
Any XX infant, no matter how virilized, should be raised as a girl to preserve the chance
of future fertility. A large, protruding clitoris should be reduced in size with a nervesparing recession or reduction rather than simple amputation.
Any undervirilized XY infant should be raised as a boy if the penis could be expected to
be large enough to stand to urinate and to insert into a vagina for coitus. If it was too
small or too malformed (e.g., cloacal exstrophy) for these functions, it was
recommended that the baby be assigned as female, any gonads removed, a vaginal
opening surgically constructed, and estrogen provided at puberty.
An infant with mixed chromosomes (e.g., mixed gonadal dysgenesis or true
hermaphroditism) could be raised either way depending on appearance of genitalia and
size of phallus.
Gender identity is set by 2 years of age and reassignment after that age should not be
attempted unless requested by the patient.
Mid 90’s
•
•
•
•
Dozens of grown intersex patients complained publicly about unsatisfactory sexual
function or incongruent gender identity, and criticized infant surgery for intersex
conditions. Some have suggested that assignments be made more tentatively and surgery
deferred in acknowledgement of the possibility of a desire to change gender when the
child is older (see Re-assignment, below)
In 1997, the "rest of" David Reimer’s story was made public. He was the boy who had
lost his penis to a surgical accident at 8 months in 1966, was reassigned from boy to girl
at 18 months with further surgery to remove testes and estrogen treatment beginning at
age 12. Although John Money had described the reassignment as a success in the 1970s,
Reimer went public with his account of continuing to have a male gender identity
despite the reassignment to a female sex of rearing. At age 15, Reimer reverted to living
as a male. At age 38, he committed suicide.
There has been a significant swing in educated opinion back toward the importance of
biological factors ("nature") in many aspects of human sexuality.
A large proportion of XY infants born with Cloacal extrophy and raised as female from
early infancy have requested reassignment to male gender in late childhood and
adolescence.
Today’s recomendations
•
•
•
•
Raise nearly all XX infants with functional ovaries as female.
– The only rare exception would be completely and unambiguously virilized XX
infants with Congenital Adrenal hyperplasia, who might be raised as male with
genital surgery deferred.
Raise most ambiguous XY infants with testes as male unless the external genitalia are
more female than male, marked androgen insensitivity is present, and testes are absent
or defective.
– Raise as male any biological male with unambiguous micropenis.
– Raise as male any XY infant with functional testes and normal androgen sensitivity
but malformed or absent penis.
Raise infants with mixed gonadal tissue, true hermaphroditism, or other chromosomal
abnormalities as the sex most consistent with external genitalia, since gonads are usually
nonfunctional.
Gender identity is set by 1-2 years of age and reassignment after that age should not be
attempted unless requested by the patient.
Gender reassignment
• http://www.youtube.com/watch?v=QeSvkE
9ZtHk
• Surgery
Biological indicators
homosexuality
Homosexuality has multiple causes
• Genetic
• Hormonal
• Immunological
Genetic evidence
Bailey & Pillard
Dean Hamer and the Xq28
Genetic Markers
• Hamer studied 40 pairs of homosexual
brothers, and reported that 33 pairs shared a
set of five X-linked genetic markers.
Fingerprints
Gays and lesbians are
also more likely to be
left handed
Both fingerprint patterns and Left-handedness are genetically determined
Gender differentiation period
From: MacLusky and Naftolin, 1981
Animal
Gestation or Incubation
Rat
Mouse
Guinea Pig
Sheep
Rhesus monkey
Zebra finch
20 – 22
19 – 20
63 – 70
145
146 – 180
12 - 14
Critical Period
18 – 27 days
Postnatal
30 – 37 days
30 – 90 days
40 – 60 days
posthatching
Brain Differentiation Rats
Gender differentiation brain
INAH3 was found to be 3 times smaller in homosexual males
Older brother effect
• each older brother increases a man's odds of
developing a homosexual sexual orientation
by 28%–48%