Insulin
advertisement

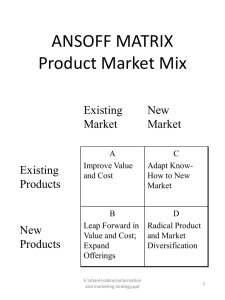
METABOLISM OF GLUCOSE AND ITS DISTURBANCES, GLYOGENOSES Lecture from Pathological Physiology © O. Rácz, A. Chmelárová & E. Lovásová school year 2012/2013 12.10.12 gluce12.ppt 1 DISORDERS OF GLUCOSE METABOLISM – OVERVIEW EXOGENEOUS SOURCES: NOT SWEET Polysaccharides: starch, glycogen (300-350 g/d); degraded in GIT by amylase, saccharidases SWEET Saccharose (sugar) lactose (milk sugar) fructose (fruit) ENDOGENEOUS SOURCES Gluconeogenesis 12.10.12 Glycogenolysis Glucose has a central role in the energetic metabolism but it is not an important component of the diet DISORDERS: Disaccharidase, lactase deficiency (malabsorption, diarrhoe) a-glucosidase blockade (treatment of obesity, type 2 diabetes) gluce12.ppt 2 THE FATE OF GLUCOSE IN CELLS 1. 2. 3. 4. 5. Glycogen synthesis. In normal postprandial state 70 – 80 g in liver, 150 g in muscles. Glycolysis and the following pathways (ATP formation) Pentose cycle (antioxidant system, pentose formation) Glucitol (sorbitol) pathway Hexosamine and uronic acid pathway 12.10.12 gluce12.ppt 3 12.10.12 gluce12.ppt 4 COMMENTS – 1 The beginning is ATP-dependent Hexokinase phosphorylates everything (different monosaccharides), entering the cell and metabolized at mininal concentrations Glukokinase in liver is glucose specific, removes postprandial glucose Glukokinase in Langerhans islets is the glucose sensor – glucokinase diabetes Hexokinase: kM 10-5, glucokinase: 10-2 (mmol/l) 12.10.12 gluce12.ppt 5 COMMENTS – 2 The main regulatory enzyme of glycolysis is the phosphofructokinase. Typical inhibitor is ATP (enough energy) Activators: AMP and fructose-2,6bisphosphate The production of 2,6-FBP in liver is increased in hyperglycaemia Glucagon inhibits its synthesis 12.10.12 gluce12.ppt 6 DISORDERS OF GLYCOLYSIS Some of them manifest as „glycogenoses“ Hereditary - congenital Phosphofructokinase deficiency – muscle fatigue Haemolytic anemias – red cell enzymopathies Acquired? Lactate acidosis: Hypoxia, pyruvatdehydrogenase deficiency, thiamin deficiency (alcoholics), As, F, Hg intoxication, sometimes in diabetes mellitus Randl cycle. Increased fatty acid oxidation (obesity, diabetes) NADH and acetylcoenzyme A overproduction. Block of glycolysis and glycogen synthesis Increased gluconeogenesis in liver… 12.10.12 gluce12.ppt 7 SEVERE (BUT RARE) DISORDERS OF MONOSACCHARIDE METABOLISM Galactosemia AR, 1/20 000 – 60 000 – Accumulation of galactose, gal-1-P, galactitol cataract, mental retardation, liver cirrhosis, haemolysis, kidney failure diet without milk Fructose intolerance AR, 1/20 000 – Accumulation of fructose & F-1-P block of glucose metabolism (glycolysis, gluconeogenesis, glycogenolysis) hypoglycaemia after sweet fruits and sweets omit them 12.10.12 gluce12.ppt 8 GALACTOSEMIA Lactose = Gal-Glu AR, 1/20 000 – 60 000, neonatal screening 12.10.12 gluce12.ppt 9 LESS SEVERE (BUT RELATIVELY COMMON) DISORDERS OF SUGAR METABOLISM Milk intolerance – opposite mutation – Lactose is important source of energy for small children – The activity of lactase is high up to age 4 years, later decreases – Milk intolerant adult people are the nonmutants – People able consume milk in adulthood are mutants – their off switch is not working – Selection according to life style – hunters contra farmers Fructosuria – Fructose does not enter into metabolism, excretion through urine 12.10.12 gluce12.ppt 10 12.10.12 gluce12.ppt 11 GLYCOGEN STORAGE DISEASES, GSD* Synthesis of glycogen (energy from ATP & UTP) – – – – G6P G1P no problem Activation with UTP UDP-glucose primer, 1-4 polymerisation & 1-6 branching after 10 20 nm particles Glycogenolysis – phosphorylase (different from amylase) makes G1P – debranching makes glucose *Originally I – VII, 2000 IX, Fernandes 2008 – more than15 12.10.12 gluce12.ppt 12 GLYCOGEN STORAGE DISEASES, GSD The control of synthase & phosphorylasde through signal systems (cAMP, Ca) and phosphorylation – dephosphorylation Postprandial state – synthase in state on (I) phosphorylase off (b) We need glucose!!! – adrenaline, glucagon cAMP, phosphokinases – Synthase off (D) phosphorylase on (a) 12.10.12 gluce12.ppt 13 CH20H H2COH O C=O HOCH CH CH20H CH20H 20H H H2COHCH0H H HC=O HC=O 2COH 2COH HCOH O O O O C=O C=O C=O HCOH HCOH HCOH HOCH HOCH HOCH HOCH HOCH CH2OH OH HCOH HCOH HCOH HCOH HCOH glycogen ÓZA FRUKTÓZA HCOHKeton HCOH HCOH HCOH d HCOH [Glu]n n = 2000 / 20000 C6H12O6 CH2OH CH2OH CH CH CH 2OH 2OH 2OH 12.10.12 GLUKÓZA FRUKTÓZA GLUKÓZA FRUKTÓZA Keton Aldehyd gluce12.ppt FRUKTÓZA Keton 14 The structure of glycogen (1-4 bonds and 1-6 branching) 12.10.12 gluce12.ppt 15 12.10.12 gluce12.ppt 16 CH 2 0H H 2C O H H C =O O C =O HCOH HOCH OCH CH 2 0H 2 0H H C O HCH H 2 C O H C H 2 0H H 2CCO =OHCH 2 0H H2C=O H C O H O O O O HCOH C =O C =O H CC=O OH H CO H HCOH HCOH CH HOCH HH OO CCH H HHOOCH C H 2 O H C H 2 O H H C OHH HCOH HH CCO O HH HHCO GLYCOGEN G LU K Ó ZA FR U K T Ó ZA H C OHHK eton HCOH HH CCO O HH A ldehyd HHCO [Glu]n n = 2000 / 20000 C 6 H 12 O6 C H2 O C H 2O H OOHH CCH H 2O HH CH HH 2O 2O Ó TÓ ZA ZA FR U KÓ TÓ ZA G LU K FR U K T Ó ZA G LU ZA FRU KÓ T ZA Ó ZA d K eton AKldehyd K eton Aldehyd eton C 6 H 12 O 6 C 6 H 12 O 6 C 6 H 12 O 6 12.10.12 gluce12.ppt 17 CH 2 0H H 2C O H H C =O O C =O HCOH HOCH HOCH CH 2 0H 2 0H H C O HCH H 2 C O H C H 2 0H H 2CCO OH =OHCH 2 0H H2C=O O O O HCOH O HCOH O C =O C =O H H CC=O OH H CO H HCOH HCOH H CH HOCH HH OO CCH H HHOOCH C H 2 O H C H 2 O H OHH C OHH HCOH HH CCO O HH HHCO GLYCOGEN G LU K Ó ZA FR U K T Ó ZA OHH C OHHK eton HCOH HH CCO O HH A ldehyd HHCO [Glu]n n = 2000 / 20000 C 6 H 12 O6 H2 O C H2 O C H 2O H HH CCH H 2O HH CH HH 2O 2O 2O KÓ TÓ ZA ZA FR UK Ó TÓ ZA G LU K FR U K T Ó ZA G LU ZA FRU KÓ T ZA Ó ZA nyd K eton AKldehyd K eton Aldehyd eton C 6 H 12 O 6 C 6 H 12 O 6 C 6 H 12 O 6 Hypoglycemia muscle fatigue, cramps 12.10.12 gluce12.ppt 18 GLYCOGEN STORAGE DISEASES, GSD THE PRINCIPLE! LIVER – GLUCOSE FOR THE BODY von Gierke (I) not a true GSD: glucose-6phosphatase deficiency, hepatomegaly, hypoglycaemia, growth retardation for low insulin (!) Cori (III) deficiency of debranching – as “I”, less severe Andersen (IV) deficiency of branching – bad prognosis Hers (VI) deficiency of phosphorylase – as “I”, less severe 12.10.12 gluce12.ppt 19 GLYCOGEN STORAGE DISEASES, GSD THE PRINCIPLE! MUSCLES – “SINGLE MINDED” No gluconeogenesis No glucose-6-phosphatase (don’t need it) Only 1 % glycogen but altogether more than in the liver “V” Mc Ardle deficiency of muscle phosphorylase without hypoglycaemia but muscle manifestation, not very severe “III”, “IV” similar GENERALIZED “II” – Pompe, heart hypertrophy, muscle hypotonia, bad prognosis (not logical) 12.10.12 gluce12.ppt 20 GLYCOGENOSES, WHICH ARE NOT “GLYCOGENOSES”, BUT MANIFEST WITH GLYCOGEN ACCUMULATION 12.10.12 gluce12.ppt 21 Glucose homeostasis Insulin lowers blood glucose (yes, but...) Insulin enables glucose metabolism in cells (yes, but...) Insulin exerts its effect through insulin receptor a transmembrane protein with kinase activity Key point of postreceptor events (a complicated cascade) is the translocation of glucose transporter GLUT4 to the membrane of muscle and fat cells THE PLAYERS OF THE GAME: 12.10.12 GLUCOSE INSULIN INSULIN RECEPTOR GLUCOSE TRANSPORTER gluce12.ppt 22 glucose IR GLUT4 12.10.12 gluce12.ppt 23 INSULIN glucose IR GLUT4 12.10.12 gluce12.ppt 24 INSULIN glucose IR GLUT4 12.10.12 gluce12.ppt 25 NO INSULIN – TYPE 1 DIABETES, PANCREATECTOMY... glucose IR GLUT4 12.10.12 gluce12.ppt 26 INSULIN RESISTANCE – PROBLEMS WITH THE RECEPTOR OR CASCADE glucose IR GLUT4 12.10.12 gluce12.ppt 27 INSULIN RESISTANCE – COMPENSATORY HYPERSECRETION OF INSULIN glucose IR GLUT4 12.10.12 gluce12.ppt 28 12.10.12 gluce12.ppt 29 Cellular Secretion of Insulin 12.10.12 gluce12.ppt 30 12.10.12 gluce12.ppt 31 Time course for insulin action Immediate increase in glucose uptake into cells (seconds) Changes in enzymatic activity (minutes) Increase in enzyme synthesis: glucokinase, PFK1, pyruvate kinaase (hours to days) glu Glucose transporter PFK1 enzyme activity Changes in gene expression 12.10.12 gluce12.ppt 32 INSULIN SECRETION IN LANGERNAS ISLETS GLUT2 – glucose transporter of B cells GK – glucokinase, glucose sensor MIT – mitochondriae, ATP production Kir6.2-SUR1 – Potassium inward rectifier channel (K-channel) with receptorom for sulphanylurea 12.10.12 gluce12.ppt 33 GLUCOSE GLUT2 GK MIT INSULIN K+ SUR1 12.10.12 Ca ++ gluce12.ppt KIR 6.2 34 GLUCOSE GLUT2 GK MIT INSULIN K+ SUR1 12.10.12 Ca ++ gluce12.ppt KIR 6.2 35 GLUCOSE GLUT2 GK MIT INSULIN K+ SUR1 12.10.12 Ca ++ gluce12.ppt KIR 6.2 36 GLUCOSE GLUT2 GK MIT INSULIN ATP K+ SUR1 12.10.12 Ca ++ gluce12.ppt KIR 6.2 37 GLUCOSE GLUT2 GK MIT INSULIN Ca ++ ATP K+ SUR1 12.10.12 gluce12.ppt KIR 6.2 38 GLUCOSE GLUT2 GK MIT INSULIN Ca ++ ATP K+ SUR1 12.10.12 gluce12.ppt KIR 6.2 39 GLUT2, GLUCOKINASE, MITOCHONDRIAE Kir6.2-SUR1 – Potassium inward rectifier channel (K-channel) – ATP INCREASE – CLOSING OF K-CHANNEL – MEMBRANE DEPOLARISATION – Ca++ ENTRY – INSULIN SECRETION 12.10.12 gluce12.ppt 40 GLUCOSE GLUT2 GK MIT INSULIN K+ SUR1 12.10.12 Ca ++ gluce12.ppt KIR 6.2 41 Insulin and its antagonists Glucagon – glycogen breakdown, gluconeogenesis glycolysis blockade in liver Adrenaline, noradrenaline – glycogen breakdown and gluconeogenesis in muscles, lactate glucose in liver Growth hormone (anabolic hormone), lipolysis, proteosynthesis Glucocorticoids – gluconeogenesis, block of proteosynthesis Thyroid hormones and oestrogens In physiological conditions synergism (counter-regulation)gluce12.ppt 12.10.12 42 Hyperglycemia = diabetes mellitus No insulin (type 1 dm, removal of pancreas, etc.) Deficient action of insulin (type 2 dm) Antagonists (glucocorticoids, adrenaline, growth hormone, gravidity) Stress (MI, stroke) 12.10.12 gluce12.ppt 43 Hypoglycemia = diabetes mellitus (?) Errors and mistakes in diabetes treatment Increased insulin sensitivity (antagonist deficiency – m. Addison, panhypopituitarism) Nondiabetic hypoglycemia (insulinoma, glycogenoses, liver failure) 12.10.12 gluce12.ppt 44 Hypoglycemia – diff. dg. Reactive & postalimentary hypoglycemia Fasting organic hypoglycemia Exogeneous hypoglycemia – in diabetics – in nondiabetics 12.10.12 gluce12.ppt 45 Reactive & postalimentary Spontaneous after meal (ANS ?) Dumping sy. (gastrectomy) Latent diabetes mellitus (???) Fructose intolerance 12.10.12 gluce12.ppt 46 Fasting organic Insulin producing tumors of L. I. Insulin (or like) producing extrapancreatic tumors Antagonist deficiency (m. Addison, hypopituitarism) Inborn errors of metabolism (pediatry) Malnutrition (severe) Liver and kidney failure Gravidity (???) 12.10.12 gluce12.ppt 47 Exogeneous Mistakes and errors in insulin treatment – overdose, exercise, omitting of meal, insufficient education Overdose of oral antidiabetics (sulfonylurea) Alcohol (both in diabetics and nondiabetics) Drugs (sulfonylurea like) 12.10.12 gluce12.ppt 48