Spafford - Clinical Electrophysiology
advertisement

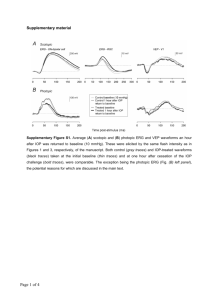
CLINICAL ELECTROPHYSIOLOGY: Plugging into the visual system Marlee M. Spafford, OD, MSc, PhD, FAAO COPE Personal Disclosure For this lecture, I have: developed the course material independently developed the course material without commercial interests no personal conflicts of interest no financial relationship with a commercial interest Basic Electrodiagnostic Equipment Specialized computer hardware & software >$100,000 Cn Pattern stimulator Ganzfeld (flash stimuli) http://www.diagnosysllc.com/home/ Visual Electrodiagnostic Tests Electroretinogram (ERG) Electro-oculogram (EOG) Visually Evoked Potential (VEP) Electroretinogram (ERG) Reflects global changes in retinal electrical potential in response to flash or pattern stimuli http://webvision.med.utah.edu/ClinicalERG.html Electro-oculogram (EOG) Records the ocular standing electrical potential Dark-adapted with light-adapted Reflects gross outer retina/RPE function + - http://brainconnection.positscience.com/med/medart/l/eye-xsection-side.gif http://webvision.med.utah.edu/ClinicalERG.html Visually Evoked Potential (VEP) Assess macular-cortical pathway’s gross integrity Record http://www.metrovision.fr http://www.aph.org/cvi/brain.html Patient #1: 6-yr-old male VEP referral (family OD): Reduced VA, not corrected by spectacles: meridional amblyopia? OD: -1.00/-3.00 x 170 OS: -2.00/-3.50 x 180 6/12 6/15 Interview: Ocular Hx: 1st Rx @ 4 yrs Nyctalopia: “always trips in the dark” Health Hx: Unremarkable Birth Hx: Polydactyl (surgery @ 1 yr) Negative family hx of eye disease 1 step-brother (“normal” vision) No parental consanguinity http://www.medes-salud.com.ar/causas.htm Nyctalopia Causes: Problem Specific Testing: Retinitis pigmentosa (RP) DFE Choroideremia Visual fields Congenital stationary night blindness (CSNB) Pan-retinal laser surgery Vitamin A deficiency Non-retinal Night myopia Optical defects (e.g., cataract) Automated > 30o; Goldmann ERG (full field ERG) Colour Vision adults; B-Y & R-G defects DFE http://www.scielo.br.proxy.lib.uwaterloo.ca/scielo.php?script=sci_arttext&pid=S0004-27492009000500019&lng=en&nrm=iso&tlng=en Bardet-Biedl Syndrome AR inheritance Cardinal Features (4 of 6) 1/179 carry gene Progressive vision loss Nyctalopia Constricted Fields Acuity loss Optometrist duties: Low vision care Referral for genetic work-up Referral to nephrologist Retinal dystrophy (RP) Polydactyly Obesity Cognitive impairment Hypogonadism Nephropathy Retinal-based Function Tests ERG Full-field ERG: fERG (typical referral) Pattern ERG: pERG Multi-focal ERG: mfERG EOG Full-field ERGs Assess the gross integrity of the outer 2/3rds of the neural retina Good test for: widespread retinal diseases vision loss that changes with lighting conditions fERG http://webvision.med.utah.edu/ClinicalERG.html fERGs Standardized fERG protocol exists: ISCEV standard: 2008 (International Society for Clinical Electrophysiology of Vision) Dark adapt (>20 min): scotopic ERGs (rod-isolated & rod-cone mixed) Light adapt (>3 min): photopic ERGs (cone-isolated) http://webvision.med.utah.edu/ClinicalERG.html Measuring fERGs a-wave: Amplitude & implicit time b-wave: Amplitude & implicit time http://webvision.med.utah.edu/ClinicalERG.html fERG Components a-wave: Photoreceptors b-wave: Müllers & On-Bipolars Oscillatory potentials (OPs): Amacrines http://webvision.med.utah.edu/ClinicalERG.html ISCEV Recording Electrodes Gold Standard Contact lens electrode (e.g., Burian-Allen Speculum Contact Lens Electrode) Bipolar electrode design CL: active Speculum: reference http://fn.bmjjournals.com/content/82/3/F233.abstract ISCEV Recording Electrodes Other ISCEV Electrodes DTL Fiber Gold foil HK loop http://www.diagnosysllc.com/products/product5.php http://www.nature.com/eye/journal/v21/n6/fig_tab/6702309f2.html DTL Fiber Electrode Insertion Ganzfeld View Chin Rest Prep ERG Recording ERG Recording Simulated fERG Normative Database (Amplitude [µV]: 20-39 yrs) R esponse S C om ponent Rod M a x im a l OPs Cone P F lic k e r 1 0 0 th 5 0 th 5 th 0 th b -w a ve b -w a ve 3 4 7 .2 7 6 8 6 .3 3 2 3 5 .1 6 4 3 7 .5 0 1 8 4 .7 7 3 1 2 .8 9 1 8 1 .6 4 2 7 7 .8 9 a -w a ve 3 6 7 .9 7 2 4 4 .1 4 1 6 2 .1 1 1 4 0 .2 4 OP2 b -w a ve 1 4 1 .4 1 2 8 6 .3 3 7 2 .6 6 2 0 3 .9 1 3 3 .5 9 1 5 2 .7 4 2 2 .6 6 1 4 3 .7 3 a -w a ve 1 5 9 .3 8 1 1 2 .1 1 7 9 .6 9 7 6 .9 6 W1 2 5 4 .3 0 1 2 3 .4 4 9 8 .8 3 8 7 .1 1 Supernormal = > 100th percentile WNL = ≥ 5th percentile Diminished = < 5th percentile Diagnostic Uses of fERG Inherited retinal disorders RPE photoreceptor disease, photoreceptor disease, chorioretinal dystrophies, vitreoretinal dystrophies Retinal ischemic disease diabetic retinopathy, central retinal vein occlusion, carotid artery stenosis, sickle cell retinopathy Pre-surgical evaluation obstructed retina due to cataract, hemorrhage or penetrating injury Retinal toxicity hydroxychloroquine Unexplained vision loss fERG: RPE-Photoreceptor Disease rod maximal flicker cone http://webvision.med.utah.edu/ClinicalERG.html fERG: Photoreceptor Disease rod maximal flicker cone http://webvision.med.utah.edu/ClinicalERG.html fERG: Photoreceptor Disease rod maximal flicker cone http://webvision.med.utah.edu/ClinicalERG.html pERG (seldom done) Reflects central retinal response (incl. ganglion cell) Macular disease Toxic/nutritional disease Unexplained central vision loss 2012 ISCEV standard http://www.diagnosysllc.com/home/ http://www.iscev.org/standards/perg.html mfERG 2011 ISCEV standard Topographical measure of outer 2/3rds of retina ~60-100 small retinal areas Local ERGs are mathematical extractions of the signal Dilated pupils; fiber electrode www.Cephalon.dk http://webvision.med.utah.edu/ClinicalERG.html Diagnostic Uses of mfERG Macular disease e.g., Stargardt Disease, ARMD Unexplained central vision loss mfERG ARMD mfERG Normal mfERG Electro-oculogram (EOG) Seldom done 2010 ISCEV standard Reflects global outer retina/RPE function Clinical diagnostic use: Best vitelliform macular dystrophy (rare, AD inheritance) EOG http://img.medscape.com/pi/emed/ckb/ophthalmology/1189694-1227128-71.jpg EOG Eyes have a ‘standing potential’ Cornea positive; RPE negative Derived from RPE; changes with retinal illumination Potential decreases in dark; increases in light Test involves: Making lateral saccades through a dark & light phases + http://www.iscev.org/standards/pdfs/eog-standard-2006.pdf - http://brainconnection.positscience.com/med/medart/l/eye-xsection-side.gif EOG Arden Ratio Light peak (LP)/dark trough (DT) >2.0: normal 1.5 to 2.0: borderline <1.5: abnormal http://www.iscev.org/standards/pdfs/eog-standard-2006.pdf Patient #2: 9-yr-old male VEP referral (family OD): Fine, mostly pendular, horizontal nystagmus, photodysphoria & reduced VA: albinism? OD: +3.00/-1.00 x 150 OS: +2.50/-0.50 x 020 6/24 6/21 Interview: Ocular Hx: Congenital nystagmus Health Hx: Unremarkable Negative family hx of eye disease/low vision No parental consanguinity http://www.kilgorevision.com/stories.htm Ocular Albinism (OA) X-linked recessive (GPR143 mutation at Xp22.3-22.2) Evidence of carrier status iris illumination ‘mud-spattered’ fundus Main Features pendular) hypopigmented skin macules Optometrist duties: Strabismus Dx/Mx Low vision care Referral for genetic work-up Sl. lighter hair & skin complexion (not necessary) Nystagmus (most horizontal & Iris tranillumination Macular hypoplasia Fundus hypopigmentation Visual pathway decussation abnormality Albinism: Problem Specific Testing Ocular Motility Iris tranillumination DFE VEP OCT (nystagmus preclude?) http://journals1.scholarsportal.info/tmp/1186526813808035824.pdf Visually Evoked Potential (VEP) Assess macular-cortical pathway’s gross integrity Record http://www.metrovision.fr NOTE: VEP = VER = VECP (latter 2: older terms) http://www.aph.org/cvi/brain.html Visually Evoked Potentials (VEPs) Types of clinical-based VEPs Pattern: pVEP 2009 ISCEV standard Full-field: fVEP 2009 ISCEV standard One example of research-based VEPs Sweep: sVEP No ISCEV standard yet VEP Stimuli pVEP fVEP NOTE: pVEPs can be reversing checkerboards or gratings http://www.metrovision.fr http://webvision.med.utah.edu/ClinicalERG.html ISCEV Recording Electrodes Scalp silver-silver chloride or gold disc surface electrodes ISCEV standard: 1 active (3 better) plus 1 reference electrode www.lkc.com VEP Electrode Placement International 10-20 system for electrode placement ISCEV Ref ISCEV Active z http://www.brainmaster.com VEP Electrode Placement Multi-channel placement Pre-chiasmal: Better Post-chiasmal: Required OZ http://www.opt.indiana.edu http://www.brainmaster.com Measuring pVEPs P100: Cortical response (Amplitude in μv) to checkerboard reversal (IT: Implicit time ~100ms) Transient VEP (<4Hz) Amp IT http://www.iscev.org/standards/pdfs/vep-standard-2004.pdf Simulated pVEP Normative Database (Implicit Time [ms]: 20-39 yrs) C h e c k S iz e 4' 8' 16' 32' 64' 128' 256' C om ponent P -1 0 0 P -1 0 0 P -1 0 0 P -1 0 0 P -1 0 0 P -1 0 0 P -1 0 0 1 0 0 th 1 2 0 .2 8 1 1 3 .2 8 1 0 1 .5 6 1 0 2 .3 4 1 0 3 .9 1 1 0 1 .5 6 1 0 1 .5 6 5 0 th 1 2 5 .0 0 1 2 2 .6 6 1 1 2 .5 0 1 0 6 .2 5 1 0 7 .8 1 1 0 9 .3 8 1 1 0 .9 4 WNL = ≤ 5th percentile Delayed = > 5th percentile 5 th 1 3 6 .7 2 1 2 8 .9 1 1 1 7 .9 7 1 1 7 .1 9 1 1 0 .9 4 1 1 4 .0 6 1 1 8 .7 5 0 th 1 4 2 .1 9 1 2 8 .9 1 1 2 1 .8 8 1 2 8 .0 0 1 1 8 .7 5 1 2 1 .8 8 1 2 0 .1 2 Measuring fVEPs P2: Cortical response to 1 Hz flash stimulus (amplitude in μv; IT: Implicit time ~100ms) fVEP useful when pVEP fails Amp IT http://www.iscev.org/standards/pdfs/vep-standard-2004.pdf Diagnostic Uses of pVEP Optic nerve disease Optic neuritis (recovery more than dx); compressive optic neuropathy; Leber’s hereditary optic neuropathy (LHON) Post-chiasmal disease (with multiple-channels) Demylinating disease; ocular albinism Amblyopia Psychogenic vision loss Unexplained vision loss Optic Neuritis http://opt.pacificu.edu/test/index.html Visual Pathway Asymmetry Albinism ~55% decussate ++ ++ ++ ~80% decussate + ++ +++ http://www.nature.com/eye/journal/v21/n10/images/6702839f3.jpg Visual Electrophysiology in Canada Specific Locations: UW Electrodiagnostic Clinic (Waterloo) UM Clinique de la Vision (Montréal) University of Ottawa Eye Institute (Ottawa) Ivey Eye Institute (London) HSC Visual Electrophysiology Unit (Toronto) St. Michael’s Hospital (Toronto) Toronto Western Hospital (Toronto) VEP only Visual Electrophysiology in Canada Other Locations? Good question! There is no Canadian registry for VE services Based on existing research activity, hospital-based, university-based VE clinical services likely exist in: Vancouver (UBC) Calgary (UofC) Edmonton (UofA) Montreal (Laval & McGill) Halifax (Dalhousie) Other cities may also provide VE services CLINICAL ELECTROPHYSIOLOGY: Plugging into the visual system Marlee M. Spafford, OD, MSc, PhD, FAAO