File
advertisement

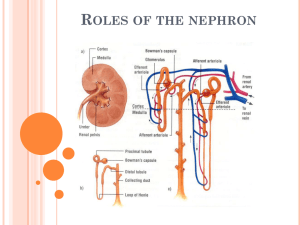
Excretion Powerpoint Urinary System Based on: Mader, S., Inquiry Into Life, McGraw-Hill Anatomy of the Kidney Based on: Mader, S., Inquiry Into Life, McGraw-Hill The Human Kidney & Nephron Urine Formation in the Nephron Urine formation in the nephron is a continuous process starting in the glomerulus and bowman’s capsule followed by the proximal convoluted tubules, loop of henle, distal convoluted tubules and finally ending in the collecting duct. Glomerulus and Bowman’s Capsule Process = Pressure filtration High blood pressure in afferent arteriole Small soluble molecules pushed out of blood through capillaries of glomerulus and collected in Bowman’s capsule Filterable - small and soluble (pass from blood into Bowman’s Capsule) Non-Filterable – large (remain in blood) “Good stuff” *** “Bad Stuff” “Good Stuff” Water Glucose Salts Amino acids vitamins Blood cells Histamines Platelets Penicillin Proteins Urea Uric acid “Bad Stuff” *** Loss of all these permanently would result in dehydration, low blood pressure, starvation and death. Proximal Convoluted Tubules Selective Reabsorption Movement of “good stuff” from the filtrate to the proximal convoluted tubules into bloodstream of the peritubular capillary network. Glucose, amino acids, vitamins, minerals Accomplished by passive transport (diffusion, osmosis, and facilitated transport) and by active transport Water is reabsorbed due to osmotic pressure caused by plasma proteins and ions in the blood Step 1: Na+ ions actively reabsorbed Step 2: Cl- ions follow passively Step 3: water moves passively into bloodstream * Threshold levels: Reabsorption occurs only until this is reached. For example, glucose has a high threshold level where as urea has a low threshold level Summary of Selective Reabsorption Reabsorbed Filtrate components Nonreabsorbed Filtrate Components (move back into bloodstream) (remain in nephron tubules) Mostly water Some water Nutrients (glucose, Nitrogenous waste amino acids) Excess salts (ions) Required salt (ions) Distal Convoluted Tubule Tubular Secretion Active transport of any unfilterable waste molecules or foreign substances (because they were too large to be originally filtered) from the blood into the distal convoluted tubules, so that these materials will become part of the urine Substance actively added to the filtrate in the distal convoluted tubules Hydrogen ions Cretinine Drugs – penicillin, histamines Loop of Henle and Collecting Duct Maintaining water-salt balance Counter-current exchange Excretion of hypertonic urine is dependent upon the reabosption of water from loop of henle collecting duct Loop of Henle, which descends into the renal medulla, is made up of two limbs; the descending limb and the ascending limb Loop of Henle NaCl diffuses out of lower portion of ascending limb Na+ is actively pumped out of upper portion of ascending limb, Cl- follow passively Ascending limb is impermeable to water, therefore water cannot move through it As a result, osmotic gradient is set up within tissues of renal medulla. The concentration of salt is greater in the direction of the inner medulla. Due to osmotic gradient between renal medulla and nephron tubules, water moves by osmosis out of both descending limb of loop of Henle and collecting duct. This movement of water out of filtrate is responsible for concentrating the urine into hypertonic solution NaCl out passively Descending Limb Increase [ ] of solute Ascending Limb NaCl out actively H2O Water comes out due to high Salinity Nephron Based on: Mader, S., Inquiry Into Life, McGraw-Hill Video Urine moves from the collecting ducts through the kidney pelvis to the ureter Based on: Mader, S., Inquiry Into Life, McGraw-Hill Incontinence (urine leakage) More than 10 million Americans experience incontinence Most do not seek treatment Treatment can improve or eliminate the problem 90% of the time Causes of Incontinence Stress incontinence: leaking small amounts of urine when coughing, lifting, or exercising Urge incontinence: the bladder suddenly and unexpectedly contracts and expels urine Overflow incontinence: bladder cannot completely empty so urine dribbles Treatments for Incontinence Kegel exercises to strengthen the urinary sphincter Medicines that increase the sphincter’s ability to contract Surgery to strengthen the pelvic muscles or to lift the bladder Retrain the bladder to increase its storage capacity (allowing 3-4 hours between urinating) Drugs to prevent urge incontinence Surgery to remove part of prostate gland if responsible for overflow incontinence Kidney stones form in the kidney pelvis. There are types of stones. •Calcium stones (most common) •Uric acid stones •Bacteria caused stones •Cystein stones Based on Mayo Clinic Health Letter Urinary Tract Infection (UTI) Second most common infection following respiratory infections UTI occur when bacteria (E. coli) from the digestive tract get into the opening of the urinary tract and multiply Bacteria first infect the urethra, then move to the bladder and finally to the kidneys UTI tend to occur more in women than men Women may have more UTIs than men because: 1) they have a shorter urethra, allowing quicker access to the bladder 2) the urethral opening is nearer the anus 3) intercourse may result in UTIs in women Based on: Harvard Medical School Family Health Guide Symptoms of UTIs Urge to urinate but only small amount of urine produced Pain and burning sensation in bladder Fever Blood in urine Diagnosis and Treatment Doctors check urine for white and red blood cells and bacteria Bacteria grown in culture to determine which antibiotic will work the best UTIs are treated with antibiotics and are often cured within 1 or 2 days Kidney Disease and Ethnicity Kidney disease 26 million Americans African Americans five times likely to require dialysis or kidney transplant Possible reasons ◦ ◦ ◦ ◦ Lack of health care Genetic component Diabetes Hypertension