Pain
Lisa B. Flatt, RN, MSN, CHPN
Definition
Complex
Subjective
Psychological
Biological
Cultural
Social factors
WHAT THE PATIENT SAYS IT IS!!!!!
Types of Pain
Acute
Chronic
Intermittent
Intractable
Malignant
Neuropathic
Phantom
Radiating
Remittent
Episodic
Acute Pain
Follows injury and goes away when it
heals
May be associated with autonomic
nervous stimulation: TC, HTN,
diaphoresis (sweat not to be confuse
with sweet ), pallor, dryness
Confirm pain prior to medicated
Chronic Pain
Prolonged disease/dysfunction
Intermittent, limited, persistent (>6mo)
Influences: environment, emotional
Three categories of chronic pain
Chronic nonmalignant -– nonprogressive or healed tissue
Chronic malignant --- cancer or
progressive disease
Chronic intractable pain --- ability to
cope with chronic pain deteriorates
Areas of ‘suffering’
Physical
Social
Spiritual
HOLISTIC CARE
Environmental
Psychosocial
Physical
Spiritual
Acute vs. Chronic Pain
Acute Pain
Trauma
Surgery
Fracture
Chronic
inflammation,
bruising
Procedural
Phantom
Chronic Pain
Marriage lol
Arthritis
Malignancy/tumor
back-chronic
Non-malignant
Neuropathy
Phantom
Pain and comparison
ACUTE
Mild to severe
Sympathetic Nervous
System responses
Increased: HR, RR, BP,
diaphoretic, dilated
pupils
Subjective
r/t tissue injury
Resolves with healing
Crying, rubbing area,
holding area
CHRONIC
Mild to severe
Parasympathetic
Nervous System
Normal VS
Dry warm skin
Pupils normal or dilated
Does not always
mention pain unless
asked
Appears withdrawn and
depressed
Pain behavior often
absent
Physiology Descriptors/Categories
Intractable; resistant to analgesia,
advanced tumors
Neuropathic; peripheral or CNS, may
be tissue related
Phantom; missing limb, spinal cord
injury (some)
More categories
Cutaneous – skin or SC tissue
Deep somatic – tendon/blood vessels,
nerves
Visceral – internal organs
Radiation and Referred
Radiating – extends from area of
insult/injury outwards – UTI,
kidney/back/urethra – chest
pain/jaw/arm
Referred pain – felt in an area that is
actually not the source – chest pain
(arteries/blood vessels/muscle);
earache (right ear hurts, left ear has
infection)
Pain Stimuli
Stimulus Type
Mechanical – trauma,
tissue, blockage duct,
tumor, spasms
Thermal – heat and/or
cold
Chemical – tissue
ischemia ( blocked
artery) – muscle spasm
Physiologic basis of
pain
Tissue damage – direct
irritation of receptors
(inflammation) –
distention of duct –
irritation on nerve
endings – chemical
stimuli – tissue
destruction –
thermosensititive –
chemical (lactic acid, K,
Mg, Na)
Gate Control Theory
Nerve fibers carrying painful stimuli to
spinal cord.
Input can be modified at spinal cord level
prior to going to the brain. Stops the sense
of pain before it goes to the brain to be
processed.
Limited amount of pain stimuli the brain
can handle at one time.
Small fibers carry pain stimuli. Large fibers
stimulate a non-noxious stimuli going
through same gate (ice pack, pain meds)
this inhibits and blocks the gate.
4 points to be modulated/reduced
Peripheral site
Spinal cord
Brain stem
Cerebral cortex
Shut out pain (neuromodulators)
Mechanoreceptors -stimulation of
fibers
Endogenous opiods
Electrical stimulation
Opiods and morphine
Normal and excessive sensory stimuli
Cerebral cortex and thalamic
inhibition
Pain in the…
Threshold -Differing perceptions of pain,
fairly uniform (sprain less painful than gall
bladder attack)
Tolerance – how much you can handle
Neuromodulators (endorphin and
enkephalin) – produced in brain, act like an
opiate, bind to opiate receptor sites,
increases pain threshold **released with
fight or flight and excessive exercise**
Pain is…Psychological and
Physical
Cognitive
Toddler- dramatic, carry on – perception, frustrated,
intolerant, fearful
Childbirth – acute, varies, helpless
Emotional- anxiety, depression, stress, frustration,
length of time/perceived time
Myths- not always drug-seeking, aging means
pain, pt not complaining they don’t have, admitting
pain is a sign of weakness, unavoidable, deserved
= bad person = sinned, resistant to med’s
Suffering – physical, psychological, emotional or
distress- chronic pain and never fully relieved ---alternative holistic methods
Pain Management Principles
Acknowledge – accept-educatemedicatePharmacological and non-pharm
Different types of med’s: NSAID’s,
ASA, Opiods, etc..
Treat the pain before it becomes
severe
0-10 – treat when? 4-5 – pt
perception
Factors Influencing Pain
Age
Gender
Culture
Religion
Physical condition at start
Support
Social
Environment
Financial
Assessment Methods to
measure/describe pain
Wong/Baker Faces
Numeric
WILDA
OPQRST
COLDERRA
Wong-Baker Scales
Happy face to sad face with
sweat/tears and blood
Adult patient 0-10
Child faces 0-5
WILDA
W=word describes pain (sharp,
stabbing, throbbing, aching)
Intensity – 0-10 or faces
Location – where is it
Duration- how long does it last
Aggravating and alleviating factors –
what makes it worse or better
OPQRST
Other s/s
Provocative/palliative – what makes it
worse or better
Quality – description
Region of pain
Severityof pain
Temporal/timing
COLDERRA
Character- sharp, burning
Onset – when did it start
Location – where it is
Duration
Exacerbation – makes it worse
Relief
Radiation
Associated s/s
Assess those things we always talk
about
Age
Sex
Emotional
Blah
Blah
blah
Assess Physical Side
Facial expression
VS
Positioning
Guarding
Striking at nurse if she touches area
that hurts
Diaphoresis
Labs
Analyze
Synthesis of the assessment
Collaborative approach to other
disciplines findings
Determine a nursing diagnosis
Acute vs. chronic
Planning
Determine desired outcomes
Step by step goal strategy
Patient centered
Realistic
SMART ER
Specific
Measurable
Attainable and action based
Realistic
Timebound
Evaluation
Reassessment
WHO (world health organization)
3 – step analgesic ladder approach
Nursing intervention – backrubs, massage,
lotion, ice and heat, distraction,
(hammer…ignoring)
Environmental – noise
Listening
******Patient Bill of Rights*******
Treat pain to the best of our ability and right to
treatment, refuse treatment, pt centered
decision making, confidentiality
Implementation
Initiate and complete plan
Work toward goal
Nursing measures/massages
Pain society usage and guidelines
CDC and NIH website on pain
Physical modifications
Accupressure – Chinese healing
system, finger pressure at certain
points, ointments, linaments,
massaging
TENS, transcutaneous electrical
nerve stimulation – prickling sensation
small stimulation ( Gate control
theory)
Environmental Modification
Stairs
Room temp
Ventilation
Fans
Assistive devices
Psychological Modifications
Cognitive behavioral therapies –
model desired behaviors, learning
theories
Biofeedback theory – teach to relax,
calm, reproduce condition of
happiness
Meditation – ‘getting out of oneself’
This is not prayer.
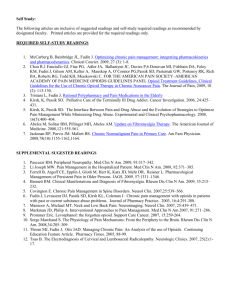
WHO 3 step Ladder
Non-opiod analygesics +/- an adjuvant.
Moderate ain persists go to
Opioid admin +/- non-opioid +/- adjuvant
Opioid for moderate to severe pain +/- non
opioid +/- adjuvant. Used for the relief of
cancer pain.
Adjuvants med’s – enhance analgesia of
opioids, treat symptoms that exacerbate
pain/provide independent analgesia for
types of pain. Corticosteroids,
antidepressants, hypnotics.
Medications/Sedatives
NSAIDS – naproxen, motrin, advil, indomethacin,
ASA, Acetaminophen
Opioids agonists – morphine, codeine,
hydromorphone, oxycodone, oxymorphine,
meperidine, fentanyl, methadone. Produce
analgesia by binding to opioid receptors.
Opioids antagonist – naloxone, reverses
depressant effect of opioids, treatm opioid OD
Opioid agonist-antagonists – pentazocine,
nalphybine, butorphanol, dezocine, bind only to
certain sites
Topical drugs localized pain
PCA
Patient controlled analgesia
Beneficial psychologically
Decreases dependency
Decreases anxiety
Patient part of their treatment plan
Evaluation
Assess verbal and nonverbal
response
Response to pain reduction methods
VS
Pain scale
MYTHS per the book
Expected with age
Chronic pain = hypochondriac
Infants feel no pain
No complaining no pain
Pain is unavoidable part of recovery
Admission is a sign of weakness
Drug addiction
Using drug at the start of pain will make it not work
as good later
Severe pain is only seen in people who are
melodramatic and/or hysterical