Shine: safety care bundle Powerpoint presentation (PPT 2.07MB)
advertisement
")
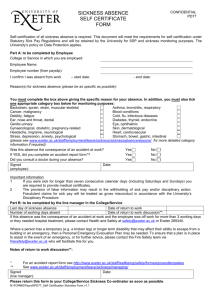
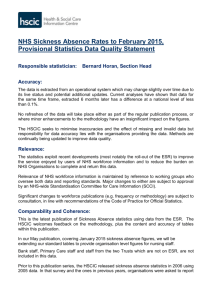
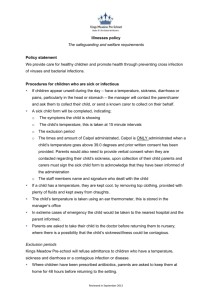
SHINE: Safety Care Bundle Health Foundation Funded Project £72,000 Norman Young Nurse Consultant, Dr Mark Haddad Clinical Research Fellow. The problem • Acute inpatient units are complex and challenging environments • As community services have expanded the severity of problems has increased. • 78% of nurses and 37% users report being subject to violence or threats (Chaplin et al 2006). • The Care Quality Commission report that 55% of mental health inpatients do not always feel safe and 16% do not feel safe at all. Effects on services: morale & performance • These stressors have an effect on the morale and performance of staff. • NHS staff have relatively high levels of sickness absence: • 10.7 days a year, • - compared to • 9.7 in public sector, • 6.4 days in private sector. Estimated incidence of self-reported illnesses caused or made worse by work in Great Britain, by illness kind, 2007/08 Stress, depression or anxiety Bone, joint or muscle problem Other type of complaint Infectious disease (virus, bacteria) Heart disease/attack, other circulatory system Breathing or lung problems 0 100 200 300 400 500 600 700 800 900 Per 100,000 workers Source: Health and Safety Executive based on Labour Force Survey Are NHS workers more stressed than other workers? Non-NHS workers NHS workers Bone, joint, muscular problem Stress, depression or anxiety Other Infectious disease Breathing or lung problem Heart disease/attack, circulatory problem 60 50 40 30 20 10 0 10 20 30 40 50 60 Percentage of workers Staff sickness Sickness absence rate* is high for mental health staff – 5.24% compared with 4.48% for the NHS (2005 data). Sickness rate ranges across different mental health trusts (1.95% – 6.91%) indicate that factors affecting sickness absence, e.g. staff injury rates, stress levels, job satisfaction, - are amenable to interventions. * dividing the total number of sickness absence days by the total number of available days Setting: Llanfair Unit •410 incident reports of aggressive or violent behaviour. •11 incidents resulting in 3 or more days of work. •1 incident more that 6 months leading to a cost of approx £42,000 • Currently average sickness cost are £119,352. •Indirect costs through increased length of stay, medication use and one to one nursing. The Intervention • There is evidence that a structured risk assessment process carried out twice a day for the first three days of admission reduce incidence of violence and aggression (Abderhalden et al, 2008) The Intervention • A tool and process were developed to systematically assess risk for all admissions • This was accompanied by ward based teaching and the use of safety briefings Evaluation questions and measures Is the care bundle associated with changes in: • • Patient safety incidents (incident reports major, minor, severe; absconding) & management of risk (special observations; forcible medication; patient restraint; patient seclusion; patient). % of individual patients/ no. episodes; Evaluation questions Bank & agency staffing. • Weekly spend; excess in relation to ward staffing budget. Staff morale & staff sickness • MBI - cross-sectional data, 2 time-points; • Number of full-time equivalent staff days lost to sickness absence; % staff members with sickness absence >7,10, 14, 21 days Evaluation questions Is the care bundle feasible & acceptable in routine practice? • • Staff interviews (semi-structured quantitative/qualitative interviews with nursing staff to examine understanding & satisfaction with intervention package). Patient questionnaires at discharge [questions adapted from NHS Mental Health Acute Inpatient Service Users Survey Questionnaire (NHS, 2008)]. Stepped Wedge Design Preliminary findings: Burnout and incidents • Sixty seven completed MBI questionnaires were returned 72% completion (n=92) • There were no statistical difference between the wards on the measure of burnout. • However higher scores for exhaustion and cynicism were evident on the ward with the highest number of incidents (116 over 12-months). Preliminary findings: Burnout and incidents • Male staff were reported more cynical attitudes than their female colleagues, this was a statistically significant difference: Independent samples t-test: t (65)=1.591, P=0.04. • Male respondents recorded slightly higher exhaustion and slightly less professional efficacy. • Band 3 and 4 staff reported highest levels of burnout (cynicism and exhaustion). • Regression analysis indicates that staff grade has a significant influence on cynicism responses when other variables are accounted for. Process and Outcome Measures U Chart of Inermittant Observations Gorwel Pre, Gorwel Post Gorwel Pre Inermittant Observations 12 Gorwel Post UCL=11.39 10 8 6 _ U=4.81 4 2 0 LCL=0 1 16 31 46 61 76 91 106 121 October 2009 to March 2011 136 151 Good Risk Management Past Tools Present Clinical Judgement Patients The Plan Risk – Male – Young age – Socially disadvantaged neighbourhoods – Lack of social support – Employment problems – Criminal peer group Childhood maltreatment History of violence First violent at young age History of childhood conduct disorder History of non-violent criminality Clinical history Psychopathy Substance abuse Personality disorder Schizophrenia Cognitive impairment Non-compliance with treatment Risk Risk Anger Impulsivity Suspiciousness Morbid jealousy Criminal/violent attitudes Command hallucinations Lack of insight Early Recognition Confused Appears to have lost their bearings; confused as to time or place or personal identity. Not limited to cognitive impairment and can include psychotic confusion. Irritable The person is easily irritated or annoyed by people or situations. The person is easily inflamed or exasperated, they have a poor tolerance to frustration. Boisterous The person is sufficiently noisy; rough; expansive to draw attention to themselves or intrudes into others personal space or “auditory space”. Early Recognition Physically threatening The person actively or passively behaves in a way that threatens another person physical well-being or causes fear of imminent attack. This includes threatening gestures, deliberately obstructing people, intruding into an individual's personal space. Verbally threatening The use of language which would cause a person fear of injury or harm. This can include phrases directed at an individual or a group of people. Attacking objects The person acts in ways that could or actually causes damage to property. James a fifty five year old man is on the third day of his admission. he has been admitted for low mood. He was transfered from recovery following carbon monoxide poisoning. During the assessment period he has asked several times what day it is, and when can he go home. Another patient complained that James was in his room and would not leave saying it was his room. This led to James shouting "get out or you'll get some" and clenched his fist at him. Martin a twenty one year old man is admitted to the ward from the crisis team. He feels that God is inside him and that he has the ability to help save lives. He hears the voice of God telling him to 'go and save people'. Over the past hour Martin has been in and out of his room 7 times and in and out of the office 6 times. He is chain smoking and walking around the ward sitting for 30seconds before getting up. He does not have conversation but walks up to people and says loudly 'why am I here' 'you are wrong' 'you are bad people'. Twice he shouts 'bastards' towards the office door and once hits a table.