抗生素正確使用原則0326
advertisement

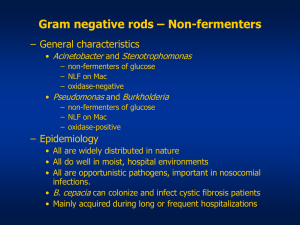
抗生素正確使用原則 張恩本醫師 為恭醫院感染科 2010.03.26 今日討論的主題 抗生素一般使用原則 抗生素 相關過敏反 應 常見的感染症致病菌 抗生素的分類 抗生素使用常見錯誤 抗素使用的適應症 常見感染症的抗生素療程 抗生素一般使用原則 Narrow spectrum 一種細菌用一種藥物治療 足量藥物治療 完整療程 使用抗生素之前應.... 用手取得檢體染色、培養 用眼觀察染色特徵 用腦社區型感染或院內感染? 想想看最可能的致病菌是什麼? 藥物敏感性如何? 理想的抗生素 Maximal damage to the bacteria, minimal damage to the host –selective toxicity Single use High effectiveness Low cost No side-effect Principles of antibiotic therapy Host factors Allergy history Age, Body weight, Renal/liver function Immune status Site of infection: pathogen, route of antibiotics Disease severity Pregnancy Empirical therapy must be adjusted after culture become available Definite antimicrobial therapy –change broadspectrum coverage to specific pathogen De-escalating therapy Pathogens of community-acquired infection Pulmonary: S. pneumoniae, H. influenzae, M. catarrhalis Skin & soft tissue: Streptococci, Staphylococci, Enterobacterioceae Intraabdomen: Enterobacterioceae, Anaerobes, Enterococci CNS: S. pneumoniae, H. influenzae, N. meningitidis Pathogens of community-acquired infection Pulmonary: S. pneumoniae, H. influenzae, M. catarrhalis Skin & soft tissue: Streptococci, Staphylococci, Enterobacterioceae Intraabdomen: Enterobacterioceae, Anaerobes, Enterococci CNS: S. pneumoniae, H. influenzae, N. meningitidis Pathogens of nosocmial infection Pulmonary: Enterobacterioceae, Pseudomonas, Acinetobacter, MRSA Intraabdomen: Enterobacterioceae, Pseudomonas, Anaerobes, Enterococci, Candida CNS: MRSA, Pseudomonas Allergic reactions to antibiotics Fixed drug eruption Skin rash (maculopapular) Exfoliativedermatitis Stevens-Johnson Syndrome (Toxic epidermal necrolysis) Anaphylactic shock Fixed rug eruption Skin rash (maculopapular) Stevens-Johnson Syndrome (Toxic epidermal necrolysis) Antibiotics Penicillins Aminoglycosides Beta-lactmase inhibitors Quinolones Cephalosporins Tetracycline Carbapenems Metronidazole Monobactams Macrolides Sulfonamides & trimethoprim Tigecycline Glycopeptide Colistimethate sodium Penicillins Natural PCNs Penicillin G, Penicillin V, benzathine PCN Penicillinase-resistant PCNs Oxacillin, Prostaphylin Amionopenicillins Amoxicillin, Ampicillin Anti-pseudomonal PCNs Ticarcillin, Piperacillin Antimicrobial spectrum of Penicillin-G Streptococcus spp. Anaerobes Neisseria spp. (Meningococcus, Gonococcus) Actinomycosis Animal bite (Pasteurella multocida) 螺旋體: Syphilis, Leptospirosis Penicillinase-resistant Penicillins oxacillin Penicillinase (β-lactamase) inhibitor Anti-staphylococcal penicillins Less active than penicillin-G against all other penicillin-susceptible microorganisms Adverse effects-PCNs Anaphylaxis, anemia, leukopenia Oxacillin: hepatitis Ticarcillin: coagulation abnormality bleeding Beta-lactam/beta-lactamatase inhibitor Sulbactam Ampicillin + Sulbactam Clavulanic acid Amoxycillin + Clavulanate Ticarcillin + Clavulanate Tazobactam Piperacillin + Tazobactam Antipseudomonal Penicillins Pip./tazo, Ticarcillin + Clavulanate Pseudomonas species Many strains of Enterobacter Anaerobics except β-lactamase producing Bacteroides species Less active against gram positive isolates Adverse effects of penicillin Anaphylaxis, anemia, leukopenia Oxacillin: hepatitis Ticarcillin: coagulation abnormality bleeding Sulbactam (Maxtam) Sulbactam is an irreversible inhibitor of betalactamase Combinations of sulbactam with beta-lactam antibiotics Dose: 0.5 ~ 1.0 gm 6 ~ 8 with other antibiotics not > 4.0 gm/day Cefoperazone/sulbactam Ampicillin/sulbactam Cephalosporins First generation Second generation Third generation Fourth generation Cephalosporins Against GPC 1st > 2nd > cephamycins > 3rd Against GNB 1st < 2nd < cephamycins < 3rd First Generation Cefazolin Cefadroxil Ceflexin Cephradine Streptococcus Staphylococcus (methicillin-susceptible) E. coli P. mirabilis K. pneumoniae Second Generation Cefmetazole Cefalor Cefuroxime Cefuroxime above the diaphragm: cefuroxime. below the diaphragm: cefmetazole (cephamycins, B. fragilis) Cefmatazole : ESBL-producing Enterobacteriaceae Third generation Cefoperazone Cefixime Cefotaxime Cefpodoxime Ceftazidime ceftibuten Ceftriaxone Flumarin Resistant Gram-negative microorganisms(Nosocomial infections) : Serratia, Citrobacter, Enterobacter, Pseudomonas, β-lactamase producing H. influenzae. Better BBB penetration among cephalosporins (except cefoperazone) Indication: nosocomial infections (mainly GNB), GNB meningitis Fourth Generation Cefepime Cefpirome Good anti-pseudomonal effect Good CNS penetration Preserve antimicrobial effect to G(+) bacteria Adverse effects of cephalosporins Cefamandole, cefmetazole, cefoperazone, cefotetan vitamin K-dependent clotting factor metabolism Monobactam (Aztreonam) Only gram-negative aerobes Alternative in penicillin- and cephalosporin- allergic patients Sulfonamides and trimethoprim Inhibit folic acid metabolism Treatment of PCP, Nocardia, Toxaplasma, Sternotrophomonus Aderverse effect: cholestatic jaudice, bone marrow suppression, severe hypersensitivity (Stevens-Johnson syndrome) Carbapenem Group Classification Group 1 Broad-spectrum carbapenems, with limited activity against non-fermentative Gram-negative bacilli (NFGNB, e.g. Pseudomonas, Acinetobacter) , that are particularly suitable for community-acquired infections (e.g. ertapenem) Group 2 Broad-spectrum carbapenems, with activity against nonfermentative Gram-negative bacilli (e.g. Pseudomonas, Acinetobacter), that are particularly suitable for nosocomial infections (e.g. imipenem and meropenem) Group3 Carbapenems with clinical activity against MethicillinResistant Staphylococcus (e.g. In development) J Antimicrob Chemotherapy Side effect of Carbapenems Anaphylaxis Interstitial nephritis Anemia Leukopenia Precipitate seizure activity, especially old patients, CRI, preexisting seizure disorder or CNS pathology Aminoglycosides Antimicrobial Spectrum: - All Gram negative bacilli - Staphylococcus aureus Dosage: - Gentamicin: loading ~ 2 mg/kg maintenance ~ 3-5 mg/kg/day Amikacin: loading ~ 7.5 mg/kg maintenance ~ 5 mg/kg Q8H or 7.5 mg/kg q12H Exacin : 8mgs/kg/day Single daily (once-daily) dosing (SDD) Short course (3-5 days) Adverse effects of aminoglycosides Nephrotoxicity Ototoxicity Neuromuscular paralysis ~ High dose/infrequent administration DECREASES the rate of tissue uptake — DELAY the onset of toxicity, doesn’t prevent it from happening ~ All patients, if treated for a long enough time, will eventually develop toxicity Fluoroquinolones Group I: - Nalidixic acid - Enteric or urinary tract infections Group II: - Ciprofloxacin, Ofloxacin, Levofloxacin - GNR (P. aeruginosa), S. pneumoniae, atypicals Group III: - Moxifloxacin, Gemifloxacin - GPB ( S. pneumoniae↑), atypicals, anaerobes, GNR (P. aeruginosa↓) - Respiratory tract infections Glycopeptides Vancomycin & Teicoplanin Non-β-lactam cell wall synthesis inhibitor Spectrum: GPC & GPB Avoid oral use, except AAC (antibiotic- associated colitis) Tetracyclines STD Rickettsial diseases - Chlamydial diseases Brucellosis - Gonorrhea Tularemia (doxycycline + ceftriaxone) - Syphilis Relapsing fever Tigecycline (a new class Glycylcyclines) Gram-positive Bacteria Gram-negative Bacteria 。Staphylococcus: MRSA, MRSE 。E. coli (including ESBLs) 。VRE: E. faecium, E. faecalis 。Kl ebsiella pneumoniae 。Streptococcus agalactiae (including ESBLs) 。S treptococcus anginosus group 。K. oxytoca 。Streptococcus pyogenes 。Acinetobacter baumannii (Resistant strains) Anaerobes 。Citrobacter freundii 。B. fragilis group 。Enterobacter cloacae 。Prevotella spp. 。Enterobacter aerogenes 。Peptostreptococcus spp. 。Stenotrophomonas maltophilia 。C. perfringens Atypical 。Chlamydia pneumoniae Does not have good activity 。Mycoplasma pneumoniae against 。Legionella P. aeruginosa Proteus. Providencia Colistimethate sodium Colistimethate sodium Pseudomonas aeruginosa infections in cystic fibrosis , multidrug-resistant Acinetobacter infection E-coli , Klebsiella sp ( ESBL) ,Enterobacter Colomycin 1,000,000 units = 80 mg colistimethate 6 to 12 mg/kg colistimethate sodium per day 60 kg man, recommended dose for Colomycin is 240 to 480 mg of colistimethate sodium Nephrotoxicity (damage to the kidneys) and neurotoxicity 抗生素使用常見的五大錯誤 Antibiotic = scanol (antipyretic) S vs R (susceptible vs resistant) 4 > 3 >2 > 1 Treat colonization Vancomycin+ imipenem(atomic bomb) Colonization Positive culture for sputum, urine, bile, stool and skin swab without symptoms or signs of infection, Not recommend for using antibiotics Except: asymptomatic bacteriuria before urological work up and in pregnancy should be treated 抗生素使用的適應症 明顯的細菌感染 極可能的細菌感染 敗血症 白血球過低合併發燒 懷疑急性心內膜炎 細菌性腦膜炎 壞死性筋膜炎 常見感染症之抗生素療程(一) 感染症療程 (天) 菌血症/敗血症 14 肝膿瘍 21 軟組織感染 7-10 急性腎炎 14 細菌性腦膜炎 10 常見感染症之抗生素療程(二) 感染症療程 (天) 肺炎雙球菌肺炎 14 (??) 革蘭氏陰性桿菌肺炎 21 (??) 退伍軍人協會症 21 奴卡氏菌肺炎 180-360 感染性心內膜炎 28-42 抗生素治療失敗之原因 選用藥物不恰當 藥物交互作用, 降低療效 異異物阻塞或膿瘍未引流 病人免疫力太差 分離菌之判讀錯誤 新的院內感染