Statins in Renal Failure
advertisement

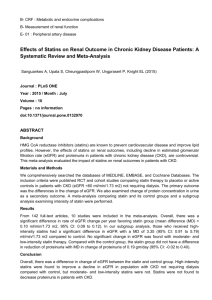
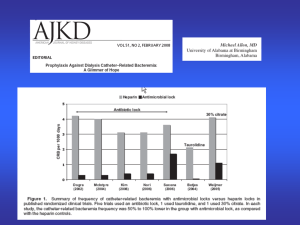
Statins in Renal Failure Andrea Fox Sunnybrook Health Science Center May 2010 No jokes No funny stories No time Objectives Discuss why the use of Statins in Stage 5 chronic kidney disease is controversial Outline the two studies that produced unexpected outcomes Provide a few practical tips from our practice at Sunnybrook HSC What is the issue? High mortality in patients on maintenance dialysis 80% have known cardiovascular disease at initiation of renal replacement therapy Have elevated CRP levels Benefits of statins in the general population are well known in cardiovascular and cerebrovascular disease- Are dialysis patients different? Expect the Unexpected Stage 3 kidney patients may receive benefit. Some evidence exists from large statin trials that included stage 3 patients that the benefit is similar or greater than the general population (post hoc subgroup analysis) Studies have not backed up assumptions that statins will reduce events and death in patients on dialysis (Stage 5) Observational studies Several observational studies have suggested that statins are associated with decreased mortality DOPPS (Dialysis Outcome and Practice Patterns Study) has shown this in 7365 prevalent hemodialysis patients Patients who used statins had 31% lower relative risk of death (p=0.0001) 23% lower cardiac mortality risk (p=0.03) 4D study The first powered RCT to address the issue: Do statins prevent CV events in dialysis patients? 1255 German patients with type 2 DM on hemodialysis Compared atorvastatin 20mg daily with placebo Composite outcome of death from cardiac causes, nonfatal MI and stroke AURORA RCT, double blind, 2776 patients aged 5080 yrs on hemodialysis Compared rosuvastatin 10mg daily with placebo Primary end point: time to major CV events (death from CV causes, nonfatal MI or nonfatal stroke) Secondary endpoints included change in lipids and CRP levels. Study comments Both trials significantly reduced LDL-C levels (43% and 42%) Both trials showed decrease in CRP in statin group vs. a rise in placebo group Statin use did NOT statistically prevent the composite primary outcome in either study AURORA-LDL lowering Primary Endpoint 4D AURORA Why no benefit? Lots of drop out/drop in in both studies AURORA excluded patients who may have benefitted most from statin therapy Statistical power A Different Patient Or… are statins truly not effective in dialysis patients? Dialysis patients are different Lipid profile (normal LDL) Extensive calcification common CV deaths are different Sudden death, arrhythmias, cardiomyopathy Atherosclerotic plaque rupture is less common Are we too late? Safety Rhabdomyolysis no increase seen in muscle related adverse events or rhabdomyolysis vs. placebo Cancer No increase in new cancer diagnoses Liver Function No increases in liver function tests or new liver disease Safety: stroke risk 4D: an increase in fatal stroke risk was seen in the atorvastatin group vs placebo (27 events vs. 13, p= 0.04) AURORA: “marginal” increase in hemorrhagic stroke in patients with DM who received rosuvastatin (12 events vs. 2, P=0.07) SHARP Study of Heart and Renal Protection 9000 patients (pre-dialysis, hemodialysis, peritoneal dialysis) Patients may have received prior statin therapy Evaluating effect of combined simvastatin/ezetimibe therapy Expected to report in 2010-11 Practically speaking… Statins are used in dialysis patients, usually initiated by other services (post MI, post stroke) We often reduce higher doses (i.e.. Atorvastatin 80mg daily reduced to 40 mg) Rosuvastatin (Crestor®) dosing: Health Canada recommends starting dose of 5 mg in patients with renal failure Monograph says 40 mg dose contraindicated in patients with Cr Cl < 30ml/minute (March 2010) Conclusion? Lowering LDL-C with statins in hemodialysis patients does not necessarily reduce CV or stroke risk CV disease in patients on chronic dialysis differs from the general population No clear answer on how to use statins in this population References Fellstrom, Jardine et al; Rosuvastatin and cardiovascular events in patients undergoing hemodialysis, NEJM 2009;360(14): 1395-1407 (AURORA) Tonelli, Shurraw; In the Literature, Commentary on AURORA study; Am J Kidney Disease, 2010;55(2):237-240 Wanner, Drane et al. Atorvastatin in patients with type 2 diabetes undergoing hemodialysis. NEJM. 2005;353(3);238-248 (4D) Mason, Bailie et al. HMG_coenzyme A reductase inhibitor use is associated with mortality reduction in hemodialysis patients. Am J Kidney Disease 2005;45(1):119-126 (DOPPS)