Virtual Ward update H&F CCG Governing Body Seminar – 3rd June

Allied Health within the
Community Independence Service
Hammersmith & Fulham
Penny Magud & Gillian McTaggart
12 th November2014
The Community Independence Service
• Is an Integrated Health & Social Care Crisis Response/Admission Avoidance Service within the community , 7 days per week
• The Service operates a ‘virtual ward’ model of case management & care coordination to avoid unnecessary institutional care
• Provides an In reach service into A & E/Medical Assessment Unit & the Older Persons
Rapid Access Clinic (OPRAC) , as well as supporting earlier discharge & providing care to facilitate discharge
• Provides an integrated Intermediate Care/Therapy Led Reablement Service for up to
12 weeks
• Is the entry point for Health & Social care services
Community Independence Service Structure 1 st November 2014
CIS service coordinator
Assistant CIS coordinator
1 WTE
Assistive
Technology
Coordinator
1 WTE
Clinical nurse specialist, older age mental health.
2 WTE
Physiotherapy
Clinical lead
1WTE
Nurse clinical lead
1WTE
SPoR coordinator
1WTE
Independent
Living
Assessment
Team Lead
1WTE
Community Independence
Assistants Team Leader
2 WTE
Occupational
Therapy Clinical
Lead
1WTE
Physiotherapy Team
6 WTE
Nursing team
6.2 WTE
Admin team
7 WTE
Community
Independence
Assistants
30 WTE
OT team
7 WTE
Assessor Group
10 WTE
In-reach Team
6 WTE
The development of the Community Independence
Service
• 3 Separate teams across Health & Social care to 1 integrated Health & Social Care
Service
• Limited Allied Health Professionals in the services, 15 clinical Allied Health Staff within the team
• Care being provided under an enabling ethos, without Allied Health oversight or governance, to a multi professional, multi provider service managed by a
Physiotherapist
• Unqualified assessing staff are now managed by an Allied Health Professional
• Health & Social Care senior leadership & oversight provided by 2 Occupational
Therapists
Core Achievements
• Implementation of a Workforce Competency framework
• Development of a pre-registration to registered career pathway
• The development of the Hybrid Worker programme - up skilling of unqualified staff providing non-invasive nursing & therapeutic programmes -
• Multiskilled competencies developed for the Social Work, Nursing staff, Occupational
Therapist’s & Physiotherapist ‘s within the service
• Increased complex patients supported in the community out of institutional care
• Increased patients whom have achieved their GOALS with the support of Therapeutic programme overseen by OT/Physio & under taken by CIA’s
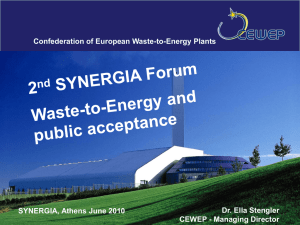
• Setting up & managing the ‘Virtual Ward’, across multiple professions & multiple providers.
Virtual Ward team
Case
Manager
GP Practice VW GP
Community
Matron
Hospital
Consultant
Other care providers community/ social/ voluntary
Patient
Health &
Social Care
Coordinator
Adult
Social
Care
Community
Independence
Service
Outcomes
• Provision of in excess of 40,000 therapeutically delivered care hours last year for 1470 patients
• 45% of patients leave the CIS with no ongoing Health & Social
Care needs
• Since April 2014, 508 ‘virtual ward’ patients have avoided an unnecessary hospital stay
• A further 468 people have been enabled to go straight home from A & E, avoiding unnecessary admission following a therapies assessment, review of their home situation & supported on the way home from Charing Cross Hospital
• 1000 bed days saved by providing a therapeutically lead in reach service enabling earlier supported discharge in 13/14