Improving Imaging Quality and Safety with e
advertisement

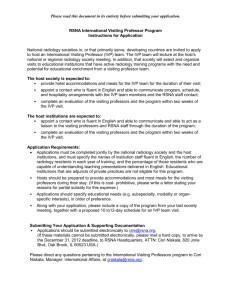
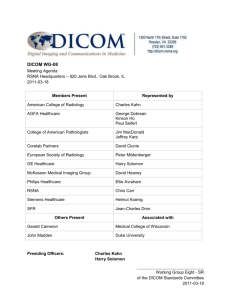
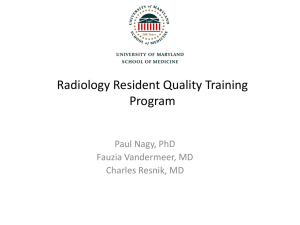
Improving Imaging Quality and safety with e-communication Ronald Arenson, MD Magnitude of the Safety Problem • 22% Americans claim family member suffered mistake Commonwealth Fund • Medical errors cause 44,000 - 98,000 deaths / year in US - IOM • Eighth leading cause of death ahead of vehicle accidents and breast cancer - AHRQ • 2% of admissions experience medication errors costing $2 billion / yr IOM • Preventable medical mistakes cost $17 - 21 billion / year - IOM • Second only to med errors, patient falls occur in 2-4% of patients and 26% result in significant injury - JCAHO Patient Care depends on Imaging • We perform procedures on many patients each day (500,000 procedures per year at UCSF) • CT and MR have become extensions of the physical examination • Triage role • Acute versus chronic • Surgical versus medical Perfect Aims to Avoid Safety Problems • Patient mis-ID • Allergy • Equipment - failure • Injection - wrong material / dose / extravasations • Reading - misinterpret • Fall - patient fall • Environment - spill • Communication • Test - wrong exam / complication / excess radiation • Metal - in magnet • Side - wrong side E-Communication • What is it? • Computer-based, non-paper, non-FAX communication • Components • • • • Web services or Service Oriented Architecture EMR note – official medical record Secure email SMS (Short Messaging Service) = Text message (with security) • “Full duplex” – acknowledgement or verification Information business • Medical Care and Radiology in particular in the information business • Access to and integration with EMR • Two major points of communication • Study requests – order entry (clinical indication) – to be discussed by Keith Dreyer, MD • Access to EMR for context, labs, meds • Reporting results – get results to our referring MDs • Make sure we have the correct target individual • Bob Wachter, MD: “Cannot do Quality and Safety without IT” Other communication challenges • Protocoling – electronic, standardization • Messages to technologists – RIS • Patient interactions • Medication / laboratory conflicts • Sending reports to patients • Management reporting: mining for quality and safety • QA “tagging” • Computer Aided Diagnosis – will not be covered in this talk • Mammography, High-res chest CT, skeletal bone age, diabetic retinopathy Patient Misidentification • Performing a procedure on the wrong patient • Giving the wrong patient injections / drugs • Technologist placing the wrong patient identifiers on images • Transcriptionist mixing up patients • Radiologist reading images for the wrong patient • RIS/PACS/transcription or voice recognition integration avoids most of these Selecting Proper Patient ID Barcode or RFID Solution • Patient ID bracelets with either barcodes or RFID • Readers associated with imaging equipment to choose from patient worklists • Portable readers for portable exams using CR which provide patient ID to plates to be read by scanners Tech worklist Select search by MRN Barcode removes other patients Appropriate Examination • Electronic Order Entry systems - CPOE • • • • • Speed transmission to Radiology May provide more patient history May improve physician and patient satisfaction Standardized order sets very helpful Can include decision-support tools that improve appropriateness • Decision-support order entry for Radiology will be in a separate presentation Reporting Communication issues • Unexpected acute findings or new neoplastic diagnosis • ACR standard for “direct” communication • “Wet readings” – wet read module • • Resident interpretations at night Accuracy and audit trail • Outside priors and curbside consults for outside studies • Poorly constructed reports – mixing up right and left, confusing abbreviations • • Smart reports – voice recognition Structured reporting • Misunderstood report findings – standard terminology like Radlex and reference information • Reporting and tracking sub-critical findings • Alex Rybkin, MD, project at SFGH Wet Read Module • Add-on to PACS • Provides immediate preliminary interpretations to ED, ICUs, others • Uses PACS displays and PDAs • Built-in feedback to referring MDs and QA for attending changes after resident interpretations Wyatt Tellis, Kathy Andriole, J Digit Imaging. 2004 Jun;17(2):80-6. Epub 2004 Mar 25 Wyatt Tellis, Kathy Andriole, J Digit Imaging. 2005 Dec;18(4):316-25 Entering wet-read Entering QA review PDA GUI Wet-Read Alert Wet-Read & Full Report Display ED Patient List RIS Query Panel Reporting errors Safely Performed • Patient Safety is a major concern for all but Radiology particularly vulnerable because • • • • we perform a very large number of procedures daily we are not very familiar with our patients there are many steps involved in the process of care we utilize drugs, contrast, radiation, needles, catheters, and other devices that can cause harm • Radiation exposure especially in CT now a major concern • Variation in dose for same examination • Large number of CT exams especially in children Protocoling Protocol GUI Scanned Requisition Radiation monitoring • Now important to capture radiation exposure from each exam (available from newer CTs / DR) • Should accumulate dose for each patient • Should share the accumulated dose with other organizations • National repository? • Requires sharing data with other institutions • RSNA contract with the NIBIB Communicating Urgent Findings • Radiologists expected to immediately communicate with referring MDs for urgent and unexpected findings • Sometimes difficult to reach referring MDs and sometimes their staff do not effectively communicate with them • Subcritical findings also a problem • Non-calcified nodule on CT, recommend f/u • Commercial systems such as VA View Alert and Vocada’s VoiceLink attempt to assist in process and documentation • Shifts responsibility away from Radiology Referring MD Miscommunication • Poor clinical history on request • No indication of reason for ordering procedure • Selection of the wrong type of procedure or the wrong side • Be sure someone talks with the patient before proceeding • Inadequate preparation of the patient for a procedure • Not reading reports carefully / no proper follow-up Communications with other institutions • In the United States, few “closed” systems, e.g. Kaiser, VA • Typical community environment • Hospitals and physicians separate entities • Incomplete or fractional EMR • Challenge of identifying patients across separate institutions and enterprises • This issue includes inpatient versus outpatient • Challenge of identifying the “relevant” clinician Management Reporting • Quality and Safety require careful monitoring • Effective management reporting is essential for this monitoring • “Dashboard” concepts can be useful in Radiology for high level view Report Turn-around Times October - Median Hours 18 16 14 12 10 8 6 4 2 0 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 Comp-Dict Prel-Final RSNA efforts • Integrating the Health Care Enterprise (IHE) • Structured Reporting • Radlex vocabulary • NIBIB Image Sharing Contract • Radiation reporting Integrating the Healthcare Enterprise IHE for Merger of Exams / Reports IHE for Processed Images IHE and Shared Context • Effective integration of separate systems requires sharing context for patient, exam, and event status • Most systems support patient ID (MRN) but do not currently support beyond that level • Radiation exposure is now an IHE profile Structured Reporting and Lexicons • Structured reporting • Can improve on the quality of communication with referring MD • Facilitates retrieval by findings / diagnosis • Provides opportunity to measure accuracy • Lexicons • BIRADS from ACR • RadLex from RSNA • RSNA now launching structured reporting project • Best practice Radiology template RadLex by RSNA • Standardized lexicon • Ontology for radiology terminology • By subspecialty • Procedures • Playbook – specific protocols rather than just CPT • Findings • Structured report and searchable terms Image sharing project • NIBIB sponsored contract with the RSNA • Six institutions sub-contracted • Patients control who has access • Avoids HIPAA issues • Uses IHE standards for image transmission • Facilitates availability of patients’ prior images when in a new institution • Technique applicable to other types of data Accumulated radiation dose Other clinical information Research data and images Hospital/Imaging Center Edge Device RIS Patient Identity Source PHR Clearinghouse PIX Manager RSNA ID Map RSNA ID Map PACS Report DB Temp Image Storage Document Source Document Registry Register Document Set [ITI4] Pid=RSNA+2nd Factor Document Repository Document Consumer Conclusions • Variety of possible patient safety problems in Radiology • Quality and Safety in Radiology can be greatly enhanced by the application of information technology • Further development and deployment of IHE are key to achieving these gains in Safety and Quality