Vitamin A and Measles
advertisement

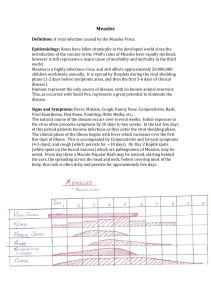
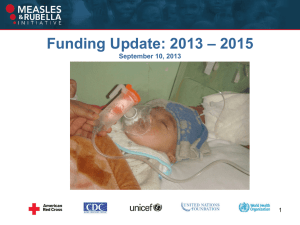
Vitamin A and Measles NSCI 5373 Mugdha Jog Vitamin A deficiency Primary Vit A deficiency: prolonged dietary deprivation, South and East Asia Secondary Vit A deficiency: interference with absorption, storage, transport of Vit A Defective absorption and storage: cystic fibrosis, celiac disease, pancreatic disease, giardiasis, cirrhosis Defective storage and transport: PEM Signs and symptoms Increased susceptibility to infections Growth retardation in children Keratomalacia Xeropthalmia Night blindness Xerosis of cornea and conjuctiva Bitots spots Diagnosis Sub-clinical stage: No evidence; history of inadequate intake Consequences of deficiency in pre-clinical stage: Increased risk of mortality from common childhood infections like diarrhea and measles Diagnosis contd Clinical stage: Shows common symptoms like xerophthalmia,etc Plasma retinol levels: good indicator Mild: 20-30 micro.gm/dl Moderate: 10-19 micro.gm/dl Severe: < 10 micro.gm/dl Diagnosis contd Plasma RBP levels: indicator Children less than or up to 10yrs: 20-30 micro.gm/ml Adult females: 42micro.gm/ml Adult males: 47micro.gm/ml Both plasma retinol and plasma RBP fall in deficient populations WHO Figures In 1995, 28 million children <5yrs of age with clinical VAD 251 million with sub-clinical VAD Under 5 mortality over 70 per 1,000 live births Xerophthalmia afflicts 2-3 million children each yr, of which 250,000 go permanently blind Recommendations Infants less than 1 yrs age:100,000 IU Children between 1-4 yrs of age:200,000 IU ( 66,000 micrograms Vitamin A palmitate in oil taken orally once every 3-6 months ). Dietary Sources Dark green leafy vegetables Yellow orange fruits: mango, papaya Liver, eggs, milk Red palm oil, cod liver oil Vitamin A fortified products: Bread, sugar, MSG, Margarine, biscuits, rice Measles Highly contagious air borne viral illness Infected children worldwide in prevaccination era Still frequent and often fatal in developing countries Measles: Pathogenesis Primary infection site- respiratory epithelium Replication in nasopharynx and regional lymph nodes Viremia- spreads to other tissues and organs Measles: Clinical Features Incubation Period: 10-12 days Prodrome: Fever, runny nose, cough, conjunctivitis Koplik’s spots Clinical Features contd Rash: 14 days after exposure Maculopapular eruptions Begins on head and face, proceeds downwards and outwards Persists 5-6 days Fades in order of appearance Other Complications Diarrhea (8%), Otitis media (7%), Pneumonia (6%), Encephalitis (0.1%), Death (0.2%) Hospitalization rate (18%) 30% cases have one or more of above Risk of death higher among children < 5yrs Treatment Medications ORT Vitamin A supplementation Immunization Immunization Live attenuated vaccine WHO recommends: 1St vaccine between 9 to 12 months of birth 2nd vaccine a month after the first one Measles in U.S Measles resurgence in U.S between 19891991 55,000 cases 45% under 5 yrs; 35% between 5-19 yrs 123 deaths ( 49% under 5yrs) 11,000 hospitalizations Reason: Low vaccine coverage Global Strategies WHO and UNICEF: Global Measles Strategic Plan. By 2005, reduce global measles deaths by 50% Achieve and maintain interruption of indigenous measles transmission with elimination goals: America(2000); Europe(2007); Eastern Mediterranean(2010) Global review and assessment of plan in 2005 Plan Strategies 1st dose by 9 months 2nd opportunity for vaccine Monitor coverage and conduct surveillance Improve measles case management Additional campaigns: Provide vitamin A supplements Include Mumps and Rubella:MMR Progress Global vaccine coverage at 70% 40% global decline in cases from 1990 to 1999 South America - measles mortality reduced by 99% 7 countries in south Africa – Measles mortality reduced by 99% just from 1996 to 1998 Conclusion Measles still accounts for 46% of the 1.7 million deaths due to vaccine-preventable diseases 30 to 40 million cases and 777,000 measles deaths still occur every year It costs less than $1 to immunize a child with the measles vaccine Children DON’T HAVE to die from measles!! Questions ?