IV CONGRESO
COLOMBIANO
DE NEFROLOGÍA
PEDIÁTRICA
Uso Prolongado de
Esteroides y
Metabolismo de
Calcio
Marco Danon, M.D.
Miami Children’s Hospital
Systemic glucocorticoids
Rheumatological
conditions
Inflammatory bowel disease
Nephrotic syndrome
Duchenne muscular dystrophy
Cystic fibrosis
Leukemia
Organ & bone marrow transplantation
Disordered puberty
Thalassemia
major
Anorexia nervosa
Gonadal damage due to
radiotherapy/chemotherapy
Klinefelter’s syndrome
Turner syndrome
Galactosemia
Childhood osteoporosis
Primary
osteoporosis
Osteogenesis imperfecta
Idiopathic juvenile osteoporosis
Osteoporosis pseudoglioma syndrome
Secondary
osteoporosis
Reduced mobility
Inflammatory cytokines
Systemic glucocorticoids
Disordered puberty
Poor nutrition/low body weight
Measurement of Bone Density
Dual energy X-ray absorptiometry (DEXA)
Direct measurement of mineral content
Indirect assessment of density
Results are affected by body size and skeletal
maturity
Does not measure trabecular density separately
Must be evaluated with pediatric software
Results must be obtained as Z-score (subject’s
results compared to age and gender – matched
controls)
DO NOT USE T-scores
Formation(+) and Resorption (-) activities during bone growth from A to B
Bone size effect on dual-energy x-ray absorptiometry scan results
Impact of bone size on dual X-ray absorptiometry measurements of BMD
Guidelines from Professional Societies
NIH Consensus Statement 2000
The International Society of Clinical
Densitometry (ISCD) recommends
evaluation of BMC and BMD for a child’s
age 2004
BMDCS (Bone Mineral Density in
Childhood Study) 2006
WHO 2007
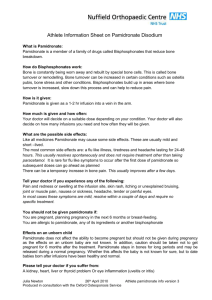
The Bone Mineral Density in Childhood Study: Bone
Mineral Content and Density According to Age, Sex,
and Race
Participants: 1554 healthy children (761 male, 793 female),
ages 6–16 yr, of all ethnicities
Objective: Establish reference curves for bone mineral
content (BMC) and density (BMD) in children
Design and Setting: The BMDC Study (measurements
annually at 5 centers in US). DXA scans by
bone densitometers
Conclusions: Age-, race-, and sex-specific reference
curves are used to identify children with bone deficits and for
monitoring bone changes in response to diseases or therapies
JCEM 92: 2087, 2007
Total hip, femoral neck, and one third radius BMD by age for non-Black (n = 603) and Black (n = 190) girls.
Smoothed curves are given for the 3rd, 25th, 50th, 75th, and 97th percentiles.
The plotted points represent the corresponding empirical percentile values for a given age group.
Glucorticoid induced Osteoporosis in Children: Crohn Disease & Nephrotic Syndrome
TABLE 2
2
The Anabolic Window
Canalis E et al. N Engl J Med 2007;357:905-916
Signals Determining Mesenchymal-Cell Differentiation toward Osteoblasts and Signals Acting
on Mature Osteoblasts to Enhance Bone Formation
Canalis E et al. N Engl J Med 2007;357:905-916
Signaling Pathways Used by Bone Morphometric Proteins in Osteoblasts
Canalis E et al. N Engl J Med 2007;357:905-916
The Canonical Wnt–β-Catenin Signaling Pathway Used in Osteoblasts
Canalis E et al. N Engl J Med 2007;357:905-916
Therapy: General Measures
Reduce or eliminate skeletal risk factors
Daily Ca & vit D. Maintain 25-OH-D above 20 ng/ml
Address underweight or obesity.
Avoid immobilization or excessive activity
Correct endogenous or iatrogenic excess of thyroid or
glucocorticoid
Sex steroid replacement for 1° or 2° hypogonadism.
Reduce activity of underlying disease. May require
glucocorticoids, methotrexate, or other osteotoxic
agents, the net benefit: reduced inflammation (cytokines
act through the receptor activator of nuclear factor[kappa]B (RANK)/RANK ligand system and ↓reduce
bone formation and increase↑bone loss similar to
glucocorticoids)
Therapy: General Measures
These general measures have proven effective
BMD increases with weight gain in patients with
anorexia nervosa, even without the return of
spontaneous menses
By contrast, sex steroids have failed to improve
BMD in randomized controlled trials to treat
anorexia nervosa in young women
For children with restricted mobility, gains in
bone mass occur with even modest increases in
skeletal loading through physical therapy or
standing on vibrating platforms
Pharmacological therapy
When failing to general measures
PTH, the most effective anabolic agent for
bone in adults, has a black box warning
against its use in children and teens,
because it has caused osteosarcoma in
growing animals.
Anticatabolic agents remain the only
pharmacological alternative for younger
patients at the present time
Growth hormone response to
prednisone dose
J Pediatr 125: 322, 1994
Bisphosphonates
Treatment for children with OI became more
widespread after iv pamidronate was shown to
reduce bone pain and fractures in an open-label
trial of 30 patients
Over the past 20 years, oral and parenteral
bisphosphonates have been used to treat OI as
well as steroid-associated osteoporosis, cerebral
palsy, muscular dystrophy, burns, idiopathic
juvenile osteoporosis, and other pediatric
disorders of bone fragility
Bisphosphonates
A Cochrane review on pediatric bisphosphonate
use for secondary osteoporosis up to 2007
807 articles, only 33 were appropriate for analysis
including 6 randomized controlled trials, 2 casecontrolled trials, 1 cohort study, and 24 case
studies or series
Because studies differed in the drugs and doses
used, the disorders treated, and the clinical
endpoints assessed, findings from the various
randomized trials could not be combined for
analysis
Bisphosphonates
Data from several pediatric trials:
BMD ↑increased in response to oral
alendronate in children after renal
transplantation and other illness requiring
glucocorticoids
By contrast, gains in BMD with
alendronate therapy in teens with anorexia
nervosa were not significantly greater than
those in patients receiving placebo after
correcting for body weight
Bisphosphonate treatment protocols for pediatric disorders
Author and year (Ref.)
Dose1
Drug
Route
Illness
Glorieux 1998 (40 )
Pamidronate
1 mg/kg · d for each of 3 d, every 4 months
iv
OI in children > age 3
Plotkin 2000 (41 )
Pamidronate
0.5–1.0 mg/kg · d for each of 3 d, every 2 to 4
months
iv
OI in children
Gandrud 2003 (60 ), Steelman
2003 (61), and Plotkin 2006
(62 )
Pamidronate
1 mg/kg (max 30 mg) every 3 months
iv
OI > age 3, idiopathic juvenile
osteoporosis, steroid-associated
osteoporosis, Duchenne muscular
dystrophy, HIV, spina bifida
Letocha 2005 (44 )
Pamidronate
10 mg/m2 · d for each of 3 d, every 3 months
iv
Children 4–16 yr of age with types III
and IV OI
Henderson 2002 (48 )
Pamidronate
1 mg/kg · d (not <15 mg or >30 mg) for each of
3 d, every 3 months
iv
Quadriplegic cerebral palsy
Acott 2005 (55 )
Pamidronate
1 mg/kg (max 90 mg) every 2 months
iv
Nephrology and rheumatology patients
DiMeglio 2006 (45 )
Alendronate,
pamidronate
Alendronate, 1 mg/kg · d (max 20 mg/d);
pamidronate, 1 mg/kg · d for each of 3 d, every
4 months
Oral, iv
Antoniazzi 2006 (47 )
Neridronate
2 mg/kg for 2 d every 3 months
iv
OI in the neonatal period
Gatti 2005 (43 )
Neridronate
2 mg/kg every 3 months
iv
OI in prepubertal children
Hogler 2004 (63 )
Zoledronate
0.25 mg/kg every 3 months
iv
Various bone disorders including
osteoporosis and avascular necrosis
Sakkers 2004 (42 ) and Kok
2007 (46 )
Olpadronate
10 mg/m 2 daily
Oral
OI with restricted ambulation
(Sakkers) and children > age 3 (Kok)
Bianchi 2000 (56 )
Alendronate
5 mg/d
Oral
Rheumatological disorders treated
with glucocorticoids
El-Husseini 2004 (49 )
Alendronate
5 mg/d
Oral
Postrenal transplantation
Golden 2005 (50 )
Alendronate
10 mg/d
Oral
Anorexia nervosa
Rudge 2005 (52 )
Alendronate
1–2 mg/kg · wk
Oral
Children with chronic illnesses
treated with glucocorticoids
Lepore 1991 (54 )
Clodronate
1200 mg daily in three divided doses
Oral
Active systemic or polyarticular
juvenile chronic arthritis
Kim 2006 (53 )
Pamidronate
125 mg/d
Oral
Nephropathy treated with
glucocorticoids
20 kg; 10 mg/d >20 kg
J Clin Endocrinol Metab 94: 400, 2009
age 2
OI in children > age 3
Choice of Bisphosphonates:
Agent and Dose
There is no consensus
Comparing outcomes: ages and diagnoses influence the
skeletal response independent of the drug or dose
employed
Dose of pamidronate to treat OI (1 mg/kg · d for 3 d
every 4 months) was extrapolated from treatment
regimens for adults with Paget’s disease
Investigators have favored a single day infusion of 1
mg/kg every 3 months
The mean annualized gain in BMD treated with the
higher-dose pamidronate regimen averaged 42% as
compared with 20% with lower doses
Adverse Effects of Bisphosphonates
in Children
An acute-phase reaction (fever, malaise, nausea, diarrhea,
and muscle or bone pain) in most children with the
initiation of iv or oral agents.
begin typically within 1-3 d of initial exposure, last only a
few days, and rarely recur with subsequent doses.
Hypocalcemia, hypophosphatemia, and hypomagnesemia
less common, typically asymptomatic, resolve within days
To reduce the risk of these deficits, adequate vitamin D
stores and calcium intake must be ensured before and
throughout bisphosphonate treatment;
using a lower initial dose of the more potent
bisphosphonate, zoledronic acid, may also be helpful (73
The more serious side effects linked to bisphosphonates in
adults such as uveitis, thrombocytopenia, or esophageal or oral
ulcerations are rare in children.
Avascular necrosis of the jaw has not been reported with
bisphosphonate therapy in any child or adolescent to date (74).
Regardless, a dental evaluation is prudent before and during
therapy in children with poor dental health.
Other concerns may be unique to the younger patient. Severe
respiratory distress has occurred with initiation of pamidronate
therapy in infants with a prior history of reactive airway disease
(75).
In teen-aged girls, there is concern for potential adverse effects
on reproductive health (76).
The half-life of alendronate and pamidronate is estimated in
years (77), and these agents can be released from bone years
after termination of therapy.
The adverse effect of greatest concern in the younger patient is
oversuppression of bone modeling and remodeling with
bisphosphonate use.
Iatrogenic osteopetrosis and pathological fractures developed in
a child treated for 2.75 yr with more than four times the high
dose (9 mg/kg · yr) of pamidronate (82).
Treatment with the standard high dose has not been shown to
delay healing of spontaneous fractures but may delay healing of
osteotomies in children with OI (83, 84).
Some investigators have hypothesized that the oscillating saw
and cautery used at surgery contribute to delayed healing in this
setting (83
Relative potency of bisphosphonates
to inhibit bone resorption
Bisphosphonates
Etidronate
Clodronate
Pamidronate
Olpadronate
Ibandronate
Alendronate
Risedronate
Zoledronate
Relative potency
1
10
100
200-500
500-1000
1000-2000
2000
10000
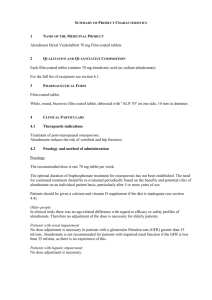
Bisphosphonate
Hypocalcemia
↑ serum
↓ bone
resorption
↓ bone pain
PTH
↓ release of Ca,
PO4, matrix
fragments and
components
Failure of normal action of
PTH, 1,25 (OH)2-vit D-bone
resorption by osteoclasts
Unopposed
anabolic actions of
PTH ± 1,25 (OH)2
– vit D on bone
↓ Remodelling
space leading to
rapid ↑ in bone
mass
↑ Exercise
Capacity
↑ Renal
retention of
Ca, ↑ renal
losses of PO4,
↑ 1,25 (OH)2vit D
↑Cortical
bone
↓bone formation at
trabecular sites
↑ bone strength,
fewer fractures
Bisphosphonate Research in Children
challenges to trials (selection of subjects and
outcome measures)
Risk to benefit ratio-favorable for children who
have already sustained vertebral or long bone
fractures
Trials are justifiable in patients with documented
longitudinal bone loss but no fractures
Define the natural history and potential for
recovery before initiating pharmacological therapy
Establishing registries for patients facing skeletal
risk factors
Treatment Summary
Controversies: Identifying child at greatest risk for fracture
General measures & treatment of chronic disease alone
uncertain
Clinicians are pressured to use bisphosphonate by anxious
colleagues or parents despite a lack of evidence
Evidence-based optimal choice of agent, dose, and duration of
treatment will require randomized, controlled trials
Until available data, conservative use of pharmacological agents
for osteoporosis is recommended.
Bisphosphonate is routine care in children with OI
For osteoporosis associated with chronic illness, bisphosphonate
is recommended only in clinical trials or compassionate for
children with ↓bone mass/density associated with low-trauma
extremity fractures and symptomatic vertebral compression
IV CONGRESO
COLOMBIANO
DE NEFROLOGÍA
PEDIÁTRICA
Albright’s dictum
Les he hablado de esteroides y calcio
mas de lo que yo mismo se
Lo que les he dicho esta sujeto a
cambio sin previo aviso
Espero que haya suscitado mas
preguntas que respuestas
De todos modos hay que investigar
mucho mas
IV CONGRESO
COLOMBIANO
DE NEFROLOGÍA
PEDIÁTRICA
Muchas
Gracias
Measurement of Bone Density
Peripheral quantitative computerized
tomography (pQCT)
Direct volumetric measurement of bone density
Results are not affected by body size
Independent and direct measurement of
trabecular compartment
Peripheral Quantitative Computerized Tomography