Steven Smith, NP
Montgomery, Alabama
CONFLICT OF INTEREST STATEMENT:
Steven Smith, NP has in years past been on the
speaker bureau for Pfizer Inc though not currently.
This CE activity was compiled without the aid of any
pharmaceutical company.
The medications and products mentioned in this
activity will be presented in a fair and balanced way.
No ink pens or coffee cups were received in
exchange for endorsement of any
pharmaceutical product mentioned in this
presentation.
WHAT IS FIBROMYALGIA SYNDROME?
Is it a musculo-skeletal disorder?
WHAT IS FIBROMYALGIA SYNDROME?
Is it a musculo-skeletal disorder?
Is it a mental condition or is it all in their heads?
WHAT IS FIBROMYALGIA SYNDROME?
Is it a musculo-skeletal disorder?
Is it a mental condition or is it all in their heads?
Is it an inflammatory, rheumatologic problem?
WHAT IS FIBROMYALGIA SYNDROME?
Is it a musculo-skeletal disorder?
Is it a mental condition or is it all in their heads?
Is it an inflammatory, rheumatologic problem?
Is it an illness of the central nervous system?
FMS is thought to be an illness of the
CENTRAL NERVOUS SYSTEM
And even more, an illness of the
NEURO-ENDOCRINE SYSTEM
FMS is thought to be one of the many
CENTRAL SENSITIZING SYNDROMES
What is CENTRAL SENSITIZING SYNDROME?
Afferent (conducting inward) sensory input into
THE DORSAL HORN GANGLION
of the spinal column overwhelm the
GATED PROTECTIVE MECHANISMS
so that you get a
WIND-UP PHENOMENON.
What is a WIND-UP PHENOMENON?
It is
NEURON HYPEREXCITABILITY
with a
LOW DISCHARGE THRESHOLD
that worsens with each sensory input (pain, touch,
movement, any sensory input).
This creates an
EXAGERATED DISCOMFORT
in people with
CENTRAL SENSITIZATION SYNDROME.
FMS is thought to be one of several
CENTRAL SENSITIZING SYNDROMES.
Others include:
IRRITABLE BOWEL SYNDROME
IRRITABLE BLADDER SYNDROME
CHRONIC PELVIC PAIN
CHRONIC FATIGUE SYNDROME
CHRONIC T M J
CHRONIC HEADACHE
RESTLESS LEG SYNDROME
THERE IS OFTEN OVERLAP AMONG THESE CONDITIONS
Also overlapping with FMS are a higher prevalence of
coexisting psychopathology:
Depression
GAD/Panic Disorder
PTSD
Bipolar Disorder
Insomnia
OCD
(responds best to FMS Tx)
(responds worse to FMS Tx)
(responds worse to FMS Tx)
Pain pathways are a two-way street.
There are AFFERENT, conducting inward,
ascending pain pathways,
(Pain towards the brain) or
(Pain on a train trying to gain toward the brain)
AND
Ameliorating, inhibitory, descending pain
pathways.
(Drain the pain from the brain) or
(Train the pain to wane)
Some of the neurotransmitters involved in the
ASCENDING pain pathways are:
Substance P
Glutamate and other excitatory amino acids
Neurotrophins
Nerve Growth Factor
Brain Derived Neurotrophic Factor
These are found in higher levels in the CEREBRAL
SPINAL FLUID of patients with Fibromyalgia
Some of the neurotransmitters involved in the
DESCENDING pain pathways that inhibit pain are:
Norepinephrine
Serotonin
The metabolites of these were found to have LOWER
levels in the Cerebral Spinal Fluid of patients with
Fibromyalgia.
! WAIT !
I THOUGHT PAIN WAS A BRAIN
THING
In one FMS study, they apply painful stimuli to both FMS patients
and a normal control group while performing an MRI observing the
increased activity in the areas of the brain related to pain.
It took only half of the painful stimuli to light up these brain areas in
the FMS patients than the control group.
The FMS patients have an increase in the “gain” or sensitivity on
their CB radios OR have an increased volume control on their
MP3 players of pain.
So, what does this have to do with
PHARMACOLOGY?
To treat FMS appropriately, you must understand:
1. The Neurotransmitters you want to increase and
decrease.
2. The Receptors you want to block.
3. The Neurons that you want to control
hyperexcitability.
4. The ascending, descending, and brain
pathophysiology of the CNS of the FMS patient.
If you understand this you will also understand what
pain ameliorating therapies NOT to use.
TWO GREAT TRUTHS
You will not adequately treat what you cannot
diagnose.
Richard Sobel, MD, mentor
If you do not know how to diagnose
Fibromyalgia then this pharmacology lecture
is useless.
Steven Smith, NP, mentee
FIBROMYALGIA is a diagnosis of EXCLUSION.
That is why FMS is a “Syndrome” and not a “Disease”.
There is no specific test for FMS.
Diagnosing FMS take the good old fashioned hard
work of a good
HISTORY AND PHYSICAL EXAM
(i.e.. SOAP)
HISTORY AND PHYSICAL EXAM
S.
CC, HPI, PMH, SocH, PsychH, FH, ROS
O.
PHYSICAL EXAM, DIAGNOSTIC TESTS
A.
ASSESSMENT/DIAGNOSIS
P.
PLAN
Name: _________Date:_______ Age:_39_Sex: __F__
FMS affects 3 million to 8 million people in the U.S.
Age is usually between 20 and 60 years old.
Over 80% of those diagnosed with FMS are female.
Mostly occurs in females of reproductive age.
S - SUBJECTIVE
CHIEF COMPLAINT: Rarely “I think I have 14/18FMS”
More often:
“I’m depressed”
“I can’t sleep”
“I’m tired all the time” AND “I hurt all over”
Legitimizing statement: “I’m afraid I’m going to lose
my job.”
20% apply for disability
50% leave the workforce
HISTORY OF PRESENT ILLNESS
FMS
Onset/duration: “A while.”
>3 mo.
Location: “My neck and my back”
4quads
Severity: “a 6 out of 10”
Quality: “It’s hard to describe, it just hurts.”
Modifying factors:
“I was in a wreck 2 years ago.”
“My friend was killed.”
HISTORY OF PRESENT ILLNESS
Modifying factors:
“I was in a wreck 2 years ago.”
“My friend was killed.”
Modifying factors in FMS:
Acute trauma
Improper body mechanics, Abnormal posture
Infection, Inflammation
Psycho-social stressors
Metabolic imbalance
FMS
HISTORY OF PRESENT ILLNESS
Associated signs and symptoms:
“I wake up tired”, “I’m depressed”,
“My nerves are shot”, “I don’t sleep well”,
“I’m gonna lose my job”
Associated signs/symptoms in FMS:
Cognitive impairment, poor sleep, fatigue, morning
stiffness, anxiety, depression, impaired social
function, impaired occupational functioning, sexual
dysfunction
HISTORY OF PRESENT ILLNESS
Current Treatment: “Goody Powders didn’t help but I
took a friends Lortab and it helped.”
“I been on Prozac since my 1st marriage ended.”
Treatment with FMS:
Will NSAIDs help FMS?
Will SSRIs help FMS?
Will narcotics help FMS?
CURRENT MEDICATIONS:
Prozac 10mg qd
Xanax 0.5mg BID
Goody Powders
CoQ 10
Will these help Fibromyalgia pain?
PAST MEDICAL HISTORY:
Fatigue, Trauma/MVA, Insomnia, Obesity
PSYCH HISTORY:
Generalized Anxiety Disorder
Depression
Abused by 1st husband
Common comorbid psychiatric conditions with FMS:
GAD, Depression, PTSD, Bipolar Disorder
PAST SURGICAL HISTORY:
C-Section x 2
Tubal ligation
FAMILY HISTORY:
Father: IBS
Mother: Depression, Migraine
2 Children: ADHD
There is a strong genetic predisposition for FMS with
the other CENTRAL SENSITIZATION SYNDROMES
(CSS) in family members.
REVIEW OF SYSTEMS:
Constitutional:
Fever
Fatigue
Sleep apnea
Weight change
Energy level
FMS
No
70%
Inactivity
Down
REVIEW OF SYSTEMS:
Eyes:
ENT:
Pulmonary:
Cardiovascular:
FMS
r/o inflam, neuro
r/o infection
r/o infection, asthma
r/o CV disease
REVIEW OF SYSTEMS:
GI:
Abd pain
Constipation
N/V/D
Bleeding
FMS
40% have IBS symptoms
REVIEW OF SYSTEMS:
GU:
Dysuria/Frequency
Incontinence
Nocturia
FMS
r/o infection
I.C. (CSS)
r/o metabolic
Ir. Bladder Sy. (CSS)
REVIEW OF SYSTEMS:
Musculoskeletal:
Back pain
Neck pain
Arthralgias
Myalgias
FMS
Always
Always
80%
80%
Fibromyalgia pain must be AXIAL not peripheral.
Fibromyalgia pain must be in ALL 4 QUADRANTS,
NOT unilateral, NOT upper or lower.
REVIEW OF SYSTEMS:
Skin:
Rash
Dry Skin
Lesions
FMS
Butterfly/malar rash
r/o Lupus
Psoriasis/psoriatic Arth.
r/o Thyroid Dz
r/o cancer
REVIEW OF SYSTEMS:
Psychiatric:
Depression
Anxiety
Insomnia
Bipolar disorder
FMS
Highly coexistant
Highly coexistant
Highly coexistant
Highly coexistant
With FMS,
1st degree relatives of FMS patients are twice as
likely to have a mood disorder.
1st degree relatives of FMS patients has an 8 fold
risk of FMS or other CSS’s.
REVIEW OF SYSTEMS:
Neurological:
Headache
Paresthesias
RLS
CVA
Seizures
FMS
53%
35%
15%
REVIEW OF SYSTEMS:
Endocrine:
Diabetes
FMS
Always r/o
Thyroid Disease
Always r/o
Dyslipidemia
? Statins
Vasomotor Perimenopausal Symptoms
REVIEW OF SYSTEMS:
Hemo/Lymph/Immun:
Easy bruising/bleeding
Lymphadenopathy
FMS
r/o cancer
r/o cancer
infection
REVIEW OF SYSTEMS:
GYN:
Vag d/c
Bleeding
Pelvic Pain
FMS
r/o infection
r/o pregnancy
Other CSS’s are Chronic Pelvic Pain, Post C-Section
Neuropathy, Post Inguinal Repair Neuropathy.
Remember, damaged nerves can lead to a “wind-up
phenomenum”. What is #1 cause of abd. Pain?
O - OBJECTIVE
PHYSICAL EXAM:
Vital signs:
Weight:
Height
BMI
B/P
HR
RR
Temp
FMS
200
62”
37
138/88
92
16
98.2
?fever
PHYSICAL EXAM:
Alert & oriented x3
Confused
Clean
Depressed
Anxious
FMS
“Fibro fog 20%”
↓ Memory
↓ Attn. Span
↓ Task Switching
↑ with FMS &
Chronic Pain
↑ Correlation
PHYSICAL EXAM:
Eyes:
Conjunctiva
FMS
PERRLA
r/o inflammatory Dz
r/o anemia
r/o MS
EMOI
r/o neuro problems
ENT:
r/o infection
PHYSICAL EXAM:
Neck:
Supple
LAD
Thyroid
FMS
r/o infection
r/o cancer
r/o thyroid dz
A GOOD TIME TO CHECK TENDERPOINTS SINCE
MOST ARE AROUND THE NECK
Bruits
PHYSICAL EXAM:
Respiratory:
CTAB
Effort normal
Retractions
Wheezing
Crackles
FMS
r/o infection
A GOOD TIME TO CHECK TENDERPOINTS
AROUND THE BACK
PHYSICAL EXAM:
CV:
FMS
r/o fatigue cause
ABD:
r/o infection
GU:
GYN:
RECTAL:
r/o infection
r/o infection
(not a fibromyalgia tenderpoint)
PHYSICAL EXAM:
Lymph:
Cervical
Supraclavicular
Axillary
Inguinal
FMS
r/o infection & cancer
A GOOD OPPORTUNITY TO CHECK
TENDERPOINTS WITHOUT BEING TOO OBVIOUS
PHYSICAL EXAM:
Neuro:
Motor
Sensory
FMS
Weakness /?MS
Reflexes
r/o cervical, lumbar
spinal stenosis
r/o hypo/hyperthyroid
Gait
r/o MS, NPH, Parkinsn
PHYSICAL EXAM:
Musculo-skeletal:
FROM Joints
Swelling
Erythema
Laxity
FMS
Check joints for RA/OA
Check tenderpoints
PHYSICAL EXAM:
Skin:
Abnormal lesions
Face
Trunk
Extremities
FMS
Rule out infection, lupus, psoriasis→(psoriatic arthritis)
scleroderma, and other skin manifestations of other
rheumatologic diseases that could cause FMS like
pain.
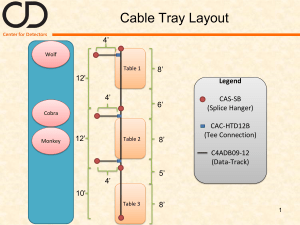
Location of FMS tender
points:
Attachment of neck muscles at
the base of the skull
Midway between neck and
shoulder
Muscle over upper inner
shoulder blade
2 cms below side bone at elbow
upper outer buttock
Hip bone
Just above knee on inside
Lower neck in front
Edge of upper breast bone
DEMONSTRATION OF PHYSICAL EXAM WITH
EMPHESIS ON FIBROMYALGIA TENDER POINTS
NEED 11 OF 18 POSITIVE TENDER POINT FOR
DIAGNOSIS OF FIBROMYANGIA
FMS affects 2-3% of the general population of the US,
4% of the female population.
The female to male “treatment seeking” ratio is 9:1
There is a 3 fold healthcare cost in FMS compared to
an average American.
SO, WHAT’S YOUR DIAGNOSIS SO FAR?
1. Family Hx of Central Sensitization Syndrome and
Psychiatric conditions
2. She has an environmental trigger: MVA with
friend killed
3. She has non-restorative sleep
4. She has a positive physical exam: 14/18 tender
points
MAYBE SHE HAS FIBROMYALGIA !
WHAT ARE YOUR DIFFERENTIAL DIAGNOSES?
1. Hormone imbalance: Hypothyroid, menstrual
irregularities, adrenal insufficiency, DM 2
2. Infection: Post infectious fatigue (Mono), Chronic
infection, Lyme Disease, HIV
3. Autoimmune D/O: Lupus, RA, PMR, Irritable
Bowel Disease
4. Neurologic: Myasthenia Gravis, Multiple Sclerosis
5. Psychiatric Illnesses: Bipolar D/O, Substance
abuse, eating d/o with malnutrition
6. Malignancies
7. Hypercalcemia (groans, stones, or bones)
What diagnostic test do you need base on your
DIAGNOSIS and DIFFERENTIAL DIAGNOSIS?
Remember, FMS is a SYNDROME, a diagnosis of
EXCLUSION.
DIAG. TESTS
RULING OUT
U/A
CBC
Pregnancy
Chem Pro
ANA
ESR
RF
CRP
TSH
CPK
Kidney dz, DM, Infection
Infection, anemia, ↓Fe, Cancer
DM, Lyte Imbal., Hypercalcemia,
Lupus
Polymyalgia Rheumatica (PMR)
Rheumatoid Arthritis
Inflammation
Hypothyroidism
Polymyositis, Muscle Damage
A - ASSESSMENT
Diagnosis: FIBROMYALGIA - Has become the #1
pain syndrome in the US.
GAD
Depression
Insomnia
h/o neck/back injury
(ALL CONTRIBUTORY)
Obesity
Tobacco abuse
P – PLAN
3 Major Goals in the treatment of Fibromyalgia
What are the 3 things you need to address and treat in
anyone with any chronic pain?
P – PLAN
3 Major Goals in the treatment of Fibromyalgia
What are the 3 things you need to address and treat in
anyone with any chronic pain?
A. TREAT PAIN
P – PLAN
3 Major Goals in the treatment of Fibromyalgia
What are the 3 things you need to address and treat in
anyone with any chronic pain?
A. TREAT PAIN
B. TREAT DEPRESSION
P – PLAN
3 Major Goals in the treatment of Fibromyalgia
What are the 3 things you need to address and treat in
anyone with any chronic pain?
A. TREAT PAIN
B. TREAT DEPRESSION
C. TREAT INSOMNIA
P – PLAN
THE TREATMENTOF FIBROMYALGIA INVOLVES:
A. Treating Fibromyalgia Pain
B. Treating Anxiety and Depression
C. Improve Sleep Architecture
P – PLAN
THE TREATMENTOF FIBROMYALGIA INVOLVES:
A. Treating Fibromyalgia Pain
B. Treating Anxiety and Depression
C. Improve Sleep Architecture
A. TREATING FIBROMYALGIA PAIN
Do you treat all pain the same?
Chest wall pain
NSAIDs
Rib fracture
Narcotics
Gout
Steroids, NSAIDs
Migraine
Triptans
Post-op pain
Narcotics
DPN/PHN
Antiepil., SNRIs,TCAs
Or, you can shoot a fly with a shotgun and give them
Lortab. NP’s are more sophisticated that that.
(5 min. to prescribe narcotics, 30 min. to explain and
treat without narcotics.)
3 TYPES OF PAIN
1. Peripheral Pain (Nociceptive):
Rib Fx, OA/RA, Gout, Trauma, Post-op
2. Neuropathic (Damaged/entrapped nerves):
DPN, PHN
3. Central Pain (Non-Nociceptive):
FMS, IBS, Ch. Pelvic Pain, other CSS’s
Can someone with RA, DPN, and drop a brick on their
foot AND have Fibromyalgia at the same time?
A. TREATING FIBROMYALGIA PAIN
Because we now know more about the
pathophysiology of Fibromyalgia pain, we will target
our approach:
1. Target ASCENDING pain pathways
2. Target inhibitory, DESCENDING pathways
Pain pathways are a two-way street.
There are AFFERENT, conducting inward,
ascending pain pathways,
(Pain towards the brain) or
(Pain on a train trying to gain toward the brain)
AND
Ameliorating, inhibitory, descending pain
pathways.
(Drain the pain from the brain) or
(Train the pain to wane)
A. TREATING FIBROMYALGIA PAIN
1. Target ASCENDING pain pathways.
HOW?
Decrease spinal neuron hyperexcitability with
anticonvulsants
a. α-2-δ (alpha-2-delta) ligand anticonvulsants
1. Pregabalin (Lyrica) – FDA approved for
Fibromyalgia
2. Gabapentin (Neurontin)
b. Other anticonvulsant/antiepileptic drugs
How does pregabalin (Lyrica) and gabapentin work?
They bind to the α-2-δ protein on the neuron that has
voltage gated channels.
A calcium ion has to go back through the gate before
certain neurotransmitters can be released from the
neuron.
How does Pregabalin (Lyrica) and gabapentin work?
(continued)
If you decrease the influx of the calcium ions, you
decrease the release of certain neurotransmitters
into the synaptic gap, therefore decreasing the
hyperexcitability of the neuron (seizure control) and,
in this case, reduce the level of Substance P and
Glutamate that play a role in pain processing and
decrease the “wind-up phenomenum” in the pain
sensing neurons.
A. TREATING FIBROMYALGIA PAIN
2. Target inhibitory, DESCENDING pain pathways.
HOW?
a. Raise Serotonin-Norepinephrine levels
1. Serotonin-Norepinephrine Reuptake Inhibitors
a. Venlafaxine (Effexor), Desvenlafaxine (Pristiq)
b. Duloxatine (Cymbalta) – FDA approved for FMS
c. Milnacipran (Savella) – FDA approved for FMS,
inhibits Norepinephrine reuptake with a 3 fold
higher potency that serotonin.
A. TREATING FIBROMYALGIA PAIN
2. Target inhibitory, DESCENDING pain pathways.
HOW?
a. Raise Serotonin-Norepinephrine levels
2. Tricyclic Antidepressants (TCAs)
a. Amitriptylline (Elavil)
b. Nortriptylline (Pamelor)
c. Imipramine
d. Others
A. TREATING FIBROMYALGIA PAIN
2. Target inhibitory, DESCENDING pain pathways.
HOW?
a. Raise Serotonin-Norepinephrine levels
3. Muscle Relaxers
a. Cyclobenzeprine (Flexeril)
A. TREATING FIBROMYALGIA PAIN
2. Target inhibitory, DESCENDING pain pathways.
HOW?
a. Raise Serotonin-Norepinephrine levels
4. Tramadol (Ultram, Ultram ER, Ultracet) – Has SNRI
properties as well as weak μ (mu) opioid-receptor
agonist properties
5. Exercise – Endorphins are pain inhibitors
A. TREATING FIBROMYALGIA PAIN
2. Target inhibitory, DESCENDING pain pathways.
HOW?
a. Raise Serotonin-Norepinephrine levels
HOW DO SNRIs WORK?
Mechanism of action is unknown
DESCENDING PAIN CIRCUITS
Hypothalamus
Periaquaductal Gray
Rostral
Ventral
Medulla
(serotonergic pathway)
Dorsolateral
Pontine
Tegmentum
(noradrenergic pathway)
Dorsolateral Funiculus
(SNRIs put the “Fun” in the Funiculus)
A. TREATING FIBROMYALGIA PAIN
2. Target inhibitory, DESCENDING pain pathways.
HOW?
a. Raise Serotonin-Norepinephrine levels
HOW?
If you can reduce the re-uptake of these
neurotransmitters back into the neuron, it leaves
more neurotransmitter in the synaptic gap leading to
pain inhibition, same as with the
antidepressant/antianxiety effect of SNRIs.
Pain pathways run through parts of the brain that tell
us where the pain is and the intensity of the pain
BUT,
Some of the pain pathways run through the areas of
the brain such as the amygdala that are related to
the affective domain or the emotional response to
pain.
This leads us to the second aspect of the treatment of
FIBROMYALGIA PAIN.
P – PLAN
THE TREATMENTOF FIBROMYALGIA INVOLVES:
A. Treating Fibromyalgia Pain
B. Treating Anxiety and Depression
C. Improve Sleep Architecture
B. TREAT ANXIETY AND DEPRESSION
1. Raise Serotonin-Norepinephrine levels
a. SNRIs
1. Venlafaxine (Effexor) – Cheaper, generic
2. Duloxatine (Cymbalta) – FDA approved for FMS
and anxiety and depression
3. Milnacipran (Savella) – FDA approved for FMS,
inhibits Norepinephrine reuptake with a 3 fold
higher potency that serotonin. You need the
serotonin reuptake inhibition to treat anxiety.
B. TREAT ANXIETY AND DEPRESSION
1. Raise Serotonin-Norepinephrine levels
b. Tricyclic Antidepressants (TCAs)
Remember: TCAs are too anticholenergic and
sedation at high enough doses to treat anxiety and
depression
B. TREAT ANXIETY AND DEPRESSION
1. Raise Serotonin-Norepinephrine levels
2. Anti-Epileptic Drugs
a. Pregabalin (Lyrica) – FDA approved for FMS,
Seizure d/o,PHN, DPN, and in Europe approved for
anxiety.
b. Gabapentin (Neurontin)
c. Valproaic Acid (Depakote)
d. Carbamazepine (Tregretol) – both used for years
for mood disorders
B. TREAT ANXIETY AND DEPRESSION
3. What NOT to use:
a. Benzodiazepines – They increase depression
and increase pain scores.
b. Narcotics – Kills a fly with a shotgun.
Morpheus – the Greek god of dreams
The Goal of Treating FMS: ECONOMIC 101
Try to get the pain scores from 6-7/10 to 2-3/10 so
they can return to work so they can pay taxes.
People addicted to benzos and narcotics tend to
take more taxes than they pay in as a rule.
P – PLAN
THE TREATMENTOF FIBROMYALGIA INVOLVES:
A. Treating Fibromyalgia Pain
B. Treating Anxiety and Depression
C. Improve Sleep Architecture
C. IMPROVE SLEEP ARCHITECTURE
80% of FMS patients report Non-Restorative Sleep.
Why do we want to improve sleep architecture?
C. IMPROVE SLEEP ARCHITECTURE
FMS polysomnographic studies show abnormalities in
sleep continuity as well as sleep architecture.
a. Decreased REM sleep with FMS
b. Increased awakenings with FMS
c. Abnormal alpha wave intrusions in non-REM which
is found to worsen pain in sleep with FMS
d. Stage 4 or Delta wave sleep is where many
restorative hormones are activated like Growth
Hormone. This leads to the fibrositis symptom
complex causing non-restorative sleep.
C. IMPROVE SLEEP ARCHITECTURE
So, poor sleep increases pain and fibrositis
symptoms.
That is why Fibromyalgia is thought to be an illness of
the NEURO-ENDOCRINE SYSTEM.
C. IMPROVE SLEEP ARCHITECTURE
1. Antiepileptic Drugs – Improve pain and sleep
a. Pregabalin (Lyrica)
1. Has a sedative effect
2. Enhances slow wave delta sleep
b. Gabapentin (neurontin)
C. IMPROVE SLEEP ARCHITECTURE
2. Tricyclic Antidepressants (TCAs) – Improve pain,
depression and sleep.
a. Amitriptylline (Elavil)
b. Imipramine (Tofranil)
c. Many others
C. IMPROVE SLEEP ARCHITECTURE
3. Non-Benzodiazepine Sedatives – Improve sleep.
a. Zolpidem (Ambien)
b. Zaleplon (Sonata)
c. Eszopiclone (Lunesta)
d. DO NOT use benzo’s
4. Teach sleep hygiene
5. Treat depression and anxiety
6. Exercising/Stretching not within 3 hours of HS
Which of the FDA approved medications would you
want to start first?
FMS pain with Fatigue dominant: Savella
FMS pain with Depression dominant: Cymbalta
FMS pain with Insomnia dominant: Lyrica
P – PLAN
THE TREATMENTOF FIBROMYALGIA INVOLVES:
A. Treating Fibromyalgia Pain
B. Treating Anxiety and Depression
C Improve Sleep Architecture
D. Other Nurse Practitioner Treatments
D. Other Nurse Practitioner Treatments
(that other healthcare providers probably won’t do)
1. Patient Education – Explain it
2. Instill a sense of self-worth
3. Avoid disability and narcotics
4. Establish anxiety reducing measures
1. Prayer
2. Exercise
D. Other Nurse Practitioner Treatments
5. Exercising and stretching – Staying active
6. Address underlying psycho-social issues and
stressors , Cognitive Behavioral Therapy (CBT)
referral.
7. Medications
8. Referral – Physical Therapy, Rheumatologist,
Neurologist, Pain Management
9. Hugs
α-2-δ (alpha-2-delta) ligand anticonvulsants
Adverse Reactions: Dizziness, somnolence, edema,
weight gain
Interactions: Potentiates other CNS drugs
Precautions: Never stop AED’s abruptly
Serotonin-Norepinephrine Reuptake Inhibitors
Adverse Reactions: Nausea, somnolence/insomnia,
constipation, dry mouth, hyperhydrosis, HTN
Interactions: Other psych meds (MAOI, SSRI, Haldol)
Precautions: Hypertension, Mania/Bipolar, Suicidal
Ideation
Tricyclic Antidepressants (TCA’s)
Adverse reactions: Drowsiness, anticholinergic
effects, Prolonged Q-T
Interactions: Anticholinergics , Prozac, MAOIs,
Alcohol/CNS depressants
Precautions: SEIZURES, Hx of seizures, Increase fall
risk and arrhythmias in Elderly, Urinary retention
Tramadol (Ultra, Ultram ER, Ultracet, Ryzolt)
Adverse Reactions: Dizziness, GI upset, Constipation,
SEIZURES
Interactions: MAOI, Carbamazepine, Alcohol
Precautions: SEIZURES, concomitant use with
opioids
Non-benzo Hypnotics
Adverse Reactions: CNS effects, Complex sleep
related behaviors
Interactions: Alcohol, CNS depressants (Marilyn
Monroe effect)
Precautions: Depression, Behavioral changes
BIG PICTURE PRECAUTIONS
SEIZURES: Tricyclic Antidepressants (TCAs),
Tramadol, and bupropion (Welbutrin) lower the
seizure threshold in people who may have never had
a seizure. Caution using together.
SEROTONIN SYNDROME: Keep in mind the doses
of concomitant use of traditional SNRIs and other
medications with SNRI effect like TCAs and
Tramadol. No need to add an SSRI.
QUESTIONS?