HRSA`s Program Integrity Initiative
advertisement

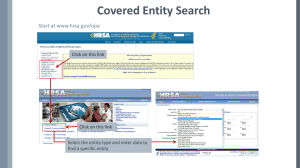
Program Integrity through 340B Compliance Hosted By: The HRSA Program Integrity Initiative Workgroup August 8, 2012 Today’s Presenters • Pat O’Rourke CFO Office • Michelle Herzog Health Services Bureau/Office of Pharmacy Affairs • Valerie Holm Office of Federal Assistance Management/Division of Financial Integrity • David Fleurquin Office of Regional Operations • Tammie Brown Office of Inspector General, HHS Agenda HRSA’s Program Integrity Initiative DHHS Office of Inspector General (OIG) National External Audit Review (NEAR) Center Introduction to the 340B Drug Pricing Program The Compliance Supplement and 340B Compliance Requirements Questions and Answers HRSA’s Program Integrity Initiative The Administrator launched the HRSA Program Integrity Initiative (PII) in June 2010. The PII was designed to: Target risks of fraud, waste and abuse Reduce risks by enhancing program integrity operations Share the best program integrity practices, and measure the results of PII efforts. Prioritized PII Actions Provide training opportunities for grantees and staff to increase program integrity Increase the number and quality of program integrity reviews and site visits conducted. Create a toolkit to facilitate collaboration and sharing of best practices. Office of Inspector General National External Audit Review Center • What is NEAR? • How does NEAR interact with DHHS sub-agencies? • How does NEAR interact with auditors? 1 HRSA’s Program Integrity Initiative An introduction to the 340B Drug Pricing Program to assist auditors who now have to test 340B compliance during the A-133 audit.. Office of Pharmacy Affairs Mission: Promote access to clinically and cost effective pharmacy services 340B Program: Overview and Benefits • Provides discounts on outpatient drugs to certain safety-net covered entities • Average savings of 25-50% Savings may be used to: Reduce price of pharmaceuticals for patients Expand services offered to patients Provide services to more patient • Estimated $6 billion dollars in 340B drug purchases last year • Manufacturers that participate in Medicaid must also participate in the 340B Program Intent of the 340B Program Permits eligible safety net providers “to stretch scarce Federal Resources as far as possible, reaching more eligible patients and providing more comprehensive services.” H.R. Rep. No. 102-384(II), at 12 (1992) Eligible Entities Federal Grantees • Comprehensive Hemophilia Treatment Centers • Federally Qualified Health Centers • Urban/ 638 Health Center • Ryan White Programs • Sexually Transmitted Disease/Tuberculosis • Title X Family Planning Hospital Types • Disproportionate Share Hospitals • Critical Access Hospitals • Rural Referral Centers • Sole Community Hospitals • Children’s Hospitals • Free Standing Cancer Hospitals 340B Enrollment Steps 1 2 3 • Determine Eligibility 4 • Complete • Submit Forms / • Await Appropriate Forms Documents to OPA Decision From OPA 340B Enrollment Deadline: October 15 January 15 April 15 July 15 Start Date: January 1 April 1 July 1 October 1 340B Enrollment Once enrolled, the newly participating entity must: Set up an account with wholesaler using 340B ID Determine if contract pharmacy services are appropriate Contact PSSC for assistance with any/ all technical issues Contact the PVP to discuss participation in their added services. Contract Pharmacies (2010 FRN (Vol. 75 No. ) • 340B program allows entities to have multiple contract pharmacies for increased patient access to cost effective pharmaceuticals • The Covered Entity purchases the drug, but “ship to - bill to” procedure may be used • The Covered Entity retains legal title to all drugs purchased under 340B. The Covered Entity must pay for all 340B drugs. 340B Database • Entities are not eligible for the program unless listed in the 340B database • Wholesalers will not ship discounted drugs unless it is an exact match to the 340B database • Information is updated daily • Includes the Medicaid Exclusion File • Online registration available for all applicants • http://opanet.hrsa.gov/opa/default.aspx Program Prohibition: Diversion • Diversion means: • a drug is provided to an individual who are not a patient of that entity • Drug dispensed in an area of a larger facility that is not eligible (e.g. an inpatient service, a non-covered clinic) • Entities should enroll all eligible outpatient or satellite sites • Required to follow patient definition guidelines 61 Fed. Reg. 55156 (October 24, 1996) Program Prohibition: Duplicate Discounts • Duplicate Discount = Accessing the 340B Discount and Medicaid Rebate on same drug • Safety-net providers required to inform HRSA at the time they enroll whether they plan to purchase and dispense 340B drugs for their Medicaid patients and bill Medicaid. • HRSA maintains this list known as the Medicaid Exclusion File on HRSA’s public website • HRSA provides guidance to covered entities and states • “Medicaid Exclusion Tutorial” and “Medicaid Exclusion File Basics” http://www.hrsa.gov/opa/medicaidexclusion.htm). • Final Notice, Duplicate Discounts and Rebates on Drug Purchases published at 58 Fed. Reg. 34058 (June 23, 1993). Recent OIG Study • State Medicaid Policies and Oversight Activities Related to 340B-Purchased Drugs – June 2011 • OIG recommendations: • CMS direct States to create written 340B policies • CMS inform States about tools they can use to identify claims for 340B-purchased drugs • HRSA share 340B ceiling prices with States. (HRSA will need to seek legislative authority to implement) • HRSA, in conjunction with CMS, improve the accuracy of the Medicaid Exclusion File 1 GAO Findings • Manufacturer Discounts in the 340B Program Offer Benefits, but Federal Oversight Needs Improvement. GAO-11-836, Sep 23, 2011 • GAO Recommendations: • Covered Entity Audits • Patient Definition • Nondiscrimination by Manufacturers • Hospital eligibility 1 ACA Provisions focusing on Program Integrity • Manufacturer Integrity (Civil Monetary Penalties) – HRSA published Advanced Notice of Proposed Rulemaking September 2010 • Covered Entity Integrity • Pricing Changes and Transparency (Regulations & on line access in 340B data system) • Administrative Dispute Resolution - HRSA published Advanced Notice of Proposed Rulemaking September 2010 • Annual on-line recertification of all entities Program Integrity - Current Activities • • • • • Determination of eligibility Annual Recertification Quarterly calculations of 340B prices Maintenance of Medicaid Exclusion File Investigations/resolutions of alleged drug diversion and incorrect pricing/inappropriate limits on drug access • Technical Assistance, webinars, FAQs, guidances Policy Releases • • • • • • Penny Pricing – Nov. 2011 Non-discrimination – Nov. 2011 Manufacturer audits – Nov. 2011 Covered entity audits – Mar. 2012 Medicaid exclusion file Hospital eligibility requirements Audits – Manufacturer Conducted • Authority • Reasonable cause • Independent auditor • Submit audit workplan to OPA for approval prior to conducting - December 12, 1996 (61 Fed. Reg. 65406) • OPA encourages manufacturers to submit plans and we will work closely with them throughout the process • OPA has received its first audit plan from a manufacturer Audits – HRSA Conducted • HRSA to date has conducted 50 of the 51 audits. • HRSA Leadership has proven commitment to this effort by providing additional auditors. • All covered entity types will be considered for audit selection, including non-HRSA grantees and hospitals • Proposed Focus Areas – Eligibility, Policies and Procedures, Internal Controls, Authorized 340B Discount, and Procurement/Distribution. A-133 plans • In addition to on-site audits, OPA has also worked closely with DFI to include 340B in the A-133 audits for all federal grantees that participate in 340B. 2012 Compliance Supplement • How do auditors know what they need to review for organizations that participate in the 340B Program? The Compliance Supplement What is the Compliance Supplement? • OMB document that is published once per year between March – June. • It is a document where the federal agencies communicate instructions to the auditor for auditing the agency’s programs. This document prevents the auditor from having to research laws and regulations for each program. What is the Compliance Supplement? • Not all programs are included in the supplement. • Federal agencies are responsible for informing OMB of any changes on an annual basis. Where Can I Find the 340B Compliance Requirements? • Since the 340B program has no CFDA number it does not have its own supplement. • The requirements for auditing 340B are found in the supplement for the applicable programs under the Special Tests and Provisions Section. Where Can I Find the 340B Compliance Requirements? Applicable Programs • For the 2012 Compliance Supplement the 340B Compliance Requirements can be found in the following program supplements: 93.224, 93.527– Consolidated Health Centers 93.917 – HIV Care Formula Grants (Ryan White, Part B) 93.918 – HIV Outpatient Early Intervention (Ryan White, Part C) Applicable Programs • The 2013 Compliance Supplement will most likely contain 340B Compliance Requirements in the following programs: 93.153 – HIV Grants for Coordinated Services (Ryan White Act) 93.217 – Family Planning - Services 93.914 – HIV Emergency Relief Project Grants (Ryan White, Part A) Suggested Audit Procedures Determine if the grantee is participating in the 340B Program and, if so, continue with the remaining audit procedures. Review the grantee’s latest change form submitted to OPA and compare it with the organization’s actual physical location and other current information about the entity. Test a sample of drugs purchased for use under the funding program (CFDA 93.xxx) during the audit period to determine whether 340B drugs were properly identified throughout the procurement process, including (1) payment at the discounted price and (2) proper identification as a 340B drug upon receipt. Suggested Audit Procedures Continued Test a sample of records of 340B drugs purchased for use under the funding program and released from inventory during the audit period to determine whether required authorizations were received, to whom the drugs were dispensed, and if the grantee determined that such individuals were eligible patients before dispensing the drugs. For eligible patients who received 340B drugs, test a sample of Medicaid reimbursement requests to verify that the grantee did not claim, receive, or retain a duplicate rebate for those drugs under the Medicaid program. Takeaways The inclusion of 340B compliance testing in the A-133 audit will increase the integrity of the 340B Program and further the efforts of the Department of Health and Human Services in preventing and detecting Fraud, Waste and Abuse in their programs.