DR RONALDA DE LACY
WHY IS IT DONE?
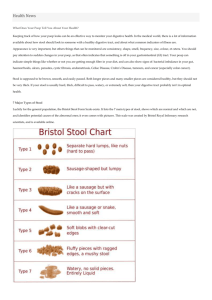
Colour
Consistency
Frequency
Blood
Bacteria
Viruses
Parasites
Fungal
Pancreatic function
Intestinal malabsorption
Inflammatory markers
STOOL COLOUR
STOOL CONSISTENCY
STOOL FREQUENCY
Breastfed infants – stool after every breastfeed
- once to twice a week
Children on average 1 to 2 stools per day
Some children might have a stool every 2nd day
BLOOD
FRESH BLOOD
Lower GIT bleed - anal fissure
- rectal haemorrhoids
- polyps
- inflammatory bowel disease
- infections i.e. Shigella, salmonella
- meckel’s diverticulum
- intussception
- NEC
BLOOD
ALTERED BLOOD (MALAENA)
Upper GIT bleed - oesophagitis
- mallory-weiss tear
- gastritis
- ulcers–gastric, duodenal, small bowel
- vascular malformations
- anastomotic sites
BACTERIA
SHIGELLA
Gram-negative rod
Nonspore forming, non-motile
Four serogroups - S. Dysenteriae (12 serotypes)
- S. Flexeneri (6 serotypes)
- S. Boydii (18 serotypes)
- S. Sonnei (1 serotype)
S. Flexeneri most frequently isolated in developing world –
60% of cases
S. Sonnei most frequently isolated in developed world –
77% of cases
SHIGELLA
BACTERIA
SALMONELLA
Gram-negative rod
Nonspore forming, motile
Many serotypes
SALMONELLA
BACTERIA
CHOLERA
Only infects humans
Transmission by faecal contamination of water and
food
Organism secretes an enterotoxin
Results in watery diarrhoea
CHOLERA
BACTERIA
CAMPYLOBACTER
Gram-negative rod- comma or S-shaped
Transmission is faecal-oral
Cattle, chickens and dogs are sources
CAMPYLOBACTER LIFECYCLE
BACTERIA
YERSINIA ENTEROLITICA
Gram-negative oval rod
Contaminated food
Enterocolitis
BACTERIA
CLOSTRIDIUM DIFFICILE
Antibiotic use
Fresh stool sample
BACTERIA
MYCOBACTERIA
Tuberculosis
Transmission by respiratory droplets
Mainly respiratory disease
Dissemination can result in intestinal involvement
Bovis
Transmission by unpasteurised cow’s milk
Intestinal involvement
Difficult to culture from stool-need tissue
VIRUS
ROTAVIRUS
RNA virus
Most common cause for diarrhoea
Vaccine available
Diagnosis antigen testing on the stool
ROTAVIRUS
VIRUS
ADENOVIRUS
DNA virus
31 antigenic types
High swinging fevers
Pneumonia
Conjunctivitis
Diarrhoea
Diagnosis – antigen testing on the stool
ADENOVIRUS
PARASITES
ENTEROBIUS VERMICULARIS
Pinworm infection
Lifecycle confined to humans
Eggs recovered from peri-anal area with tape
Adult worms may be found in the stool
ENTEROBIUS
VERMICULARIS
ENTEROBIUS VERMICULARIS(PINWORM)
PARASITES
ASCARIS LUMBRICOIDES
Transmission-eating eggs in contaminated soil
Diagnosis- oval eggs in the stool or adult worms seen
ASCARIS
LUMBRICOIDES EGG
ASCARIS LUMBRICOIDES LIFECYCLE
PARASITES
TRICHURIS TRICHURIUM
Whipworm infection
Transmission-eating eggs in contaminated soil
Diagnosis- barrel-shaped eggs in the stool
TRICHURIS
TRICHIURA
EGGS
TRICHURIS TRICHURIUM LIFECYCLE
PARASITES
TAENIA SOLIUM
Ingestion of larvae in undercooked pork
Diagnosis- proglottids in stool
gravid proglottids have 5-10 primary uterine
branches
TAENIA SAGINATA
Ingestion of larvae in undercooked beef
Diagnosis- gravid proglottids have 15-20 primary
uterine branches
TAENIA EGG
TAENIA
SAGINATA
FOUR SUCKERS
NO HOOKS
TAENIA
SOLIUM
FOUR SUCKERS
DOUBLE ROW
OF HOOKS
TAENIA LIFECYCLE
PARASITES-PROTOZOA
GIARDIA LAMBLIA
Flagellated protozoan
Waterborne transmission
Faecal-oral route
Infects the small intestine
Difficult to isolate, need minimum of 3 stool specimens
Diagnosis - trophozoites or cysts in diarrhoeal stools
- trophozoites- pear-shaped, 2 nuclei,
4 pairs of flagella, suction disk
GIARDIA
LAMBLIA
TROPHOZOITE
PARASITES-PROTOZOA
CRYPTOSPORIDIUM
Coccidian protozoa
Waterborne transmission
Direct person to person contact
Immunocompromised patients
Diagnosis- oocysts in faecal smears
CRYPTOSPORIDIUM
OOCYSTS
CRYPTOSPORIDIUM
OOCYSTS-EM
PARASITES-PROTOZOA
ENTAMOEBA HISTOLYTICA
Transmission-faecal-oral route, contaminated food
and water
Diagnosis - trophozoites in diarrhoeal stools
- cysts in formed stools – 4 nuclei
ENTAMOEBA
HISTOLYTICA
CYST
PARASITES-PROTOZOA
ISOSPORA BELLI
Faecal-oral transmission
Immunocompromised patients
Diagnosis-oocysts in faecal specimen
ISOSPORA BELLI
OOCYSTS
FUNGAL
CANDIDA ALBICANS
Part of normal gut flora
Overgrowth in diabetes, immunocompromised
patients and prolonged antibiotic use.
Diagnosis- oval yeast with a single bud in the stool
CANDIDA
ALBICANS
PANCREATIC FUNCTION
Faecal elastase
>200ug/g faeces - normal
Low in chronic diarrhoea
<15ug/g indicates pancreatic insufficiency-cystic
fibrosis
INTESTINAL MALABSORPTION
CARBOHYDRATE MALABSORPTION
Faecal reducing substances – positive – osmotic
diarrhoea
Faecal osmolar gap (FOG) – serum osmolarity2x(faecal sodium + potassium concentration)
FOG >100 mosm/l – osmotic diarrhoea
FOG <100 mosm/l – secretory diarrhoea
Need a liquid stool
INTESTINAL MALABSORPTION
PROTEIN MALABSORPTION
Stool alpha 1 anti-trypsin
Need a pre-weighed container
Clearance rate 0.8-5.4ml/24hrs
INTESTINAL MALABSORPTION
FAT MALABSORPTION
3 day faecal fat measurement
Histology- free fat
Steatocrit-not specific for free fat
INFLAMMATORY MARKERS
COLPROTECTIN
Calcium and zinc binding protein
Accounts for 30-40% of neutrophil cytosol
Resistant to enzymatic degradation
Strongly correlated with 111-indium labelled leucocytes
References range- upper limit
2-9yrs – 166ug/g faeces
10-59yrs- 51 ug/g faeces