Bowel Workshop
Alison Bardsley – Continence Advisor and
Continence Service Manager, Oxon.
Clinical Director – Continence UK
Supported by an educational grant from
Function of the Large Bowel
• Storage of food prior to elimination
• Absorption of remaining water, electrolytes
and some vitamins
• Synthesis of Vitamin K and some
Vitamin B by colonic bacteria
• Secretion of mucus to lubricate the faeces
• Elimination of food residual
How to Know when it’s time to ‘go’
•
•
•
•
•
•
•
•
Faeces move from sigmoid colon into the rectum
Full rectum
Adopt correct posture
Raise intra-abdominal pressure
Internal and external anal sphincters relax
Rectum contracts to expel stool
Should pass soft formed stool with minimal effort
Sphincter “snaps shut” after completion
THE IDEAL BOWEL MOVEMENT
• The feeling you want to go is definite but not irresistible
• Once you sit on the toilet there is no delay
• No conscious effort or straining
• The stool glides out smoothly & comfortably
• Followed by a pleasant feeling of relief
Have a Look
•
•
•
•
•
•
•
Change in ‘normal’ bowel habit persistent for 6 weeks
Undiagnosed rectal bleeding
Undiagnosed rectal pain
Blood/slime in stool
Accompanying abdominal pain/vomiting
Anorexia and weight loss
Suspected infected stool
*Refer to national colorectal cancer screening guidelines
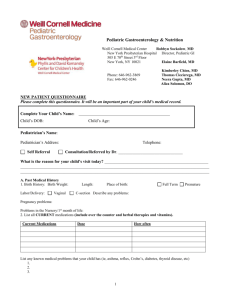
BRISTOL STOOL FORM SCALE*
Type 1:
Type 2:
Type 3:
Type 4:
Type 5:
Type 6:
Type 7:
9
Hard lumps like nuts
Lumpy sausage
Sausage with
cracked surface
Sausage with
smooth surface
Soft blobs with
well-defined margins
Fluffy with ragged
edges
Watery, no solid pieces * Reproduced by kind permission of Dr Ken Heaton, Bristol University.
Risk factors for Constipation
•
•
•
•
•
•
Medical condition
Medication
Toileting facilities
Mobility
Nutritional intake
Fluid Intake
Diet
Fibre softens stools and speeds transit
Caffeine stimulates the gut
Artificial sweeteners can cause diarrhoea
Advice on fibre moderation if stool loose or
increase if hard
Gradual caffeine reduction
Look for sensitivities in diet
Fibre don’t over do it
Dietary Fibre:
18-30g per day
Fluid Intake:
1.5 to 2 litres per day
Fruit and vegetables:
5 portions per day
Introduce fibre
gradually
if in doubt,
liaise with dietician
for specialist advice
Insoluble & Soluble Fibre
• Insoluble - bulking (laxative) agents help
prevent constipation
– Examples: Oats, fruit, vegetables and pulses
• Soluble – help reduce blood cholesterol
levels & can help control blood sugar
levels
– Examples: Wholegrain cereals and
wholemeal bread
What about laxatives?
Choice of agent will depend
on
• Presenting symptoms
• Nature of complaint
• Efficacy
• Side –effects
• Speed of action
• Patient acceptability
• Compliance
• Cost
Types of laxatives
• Bulk forming
– Fybogel®, Celvevac® Normacol®, Regulan®
Relieve constipation by increasing faecal
mass which stimulates peristalsis
Usually work within 24 -36 hours
Stimulant Laxatives
• Senna, Bisacodyl, co-danthramer, codanthrasate, dioctyl, docusol
Stimulate an increase in colonic motility
(peristalsis) and mucus secretion
Rapid acting 8-12 hours
Faecal Softener
• Liquid paraffin, arachis oil
Lubricate and soften faeces to promote a
bowel movement by lowering surface
tension of colonic contents and allowing
fat and fluid to penetrate.
Osmotic/iso-osmotic Laxatives
• Lactulose and Magnesium salts – Osmotic
Act by drawing fluid from the body into the bowel by
osmosis
• MOVICOL® - iso-osmotic
MOVICOL increases stool water content and directly
triggers colonic propulsive activity and defaecation.
4 in 1 mode of action: Bulks, softens, stimulates and
lubricates.
Enemas & Suppositories
• Phosphate, Sodium citrate, Bisacodyl,
Glycerine
Uses:
Acute or severe constipation
Retention or evacuation
Stimulation or lubricant
NEUROLOGICAL DISEASE
• Most patients will have a degree of
dysfunction or suffer from constipation
• Caused by:– Loss of mobility
– Constipating medication
– Obstetric trauma
– Anal sphincter mechanism impairment
– Dysphagia
– Cognitive problems
– Inadequate care & facilities
– Lack of understanding of care needs
AUTONOMIC DYSREFLEXIA
Unique to spinal injury above T6
SYMPTOMS
Headaches
Severe hypertension
Flushing above the lesion
Sweating below the lesion
Blotching of the skin
Nasal congestion
Bradycardia / tachycardia
Palpitations
Dilation of the pupils
SYMPTOMS
Headaches .
Severe hypertention
Flushing above the lesion
Sweating below the lesion
Blotching of the skin
Nasal congestion
Bradycardia / tachycardia
Palpitations
Dilation of the pupils
TREATMENT
•
•
•
•
•
Acute medical emergency
Remove the offending stimulus eg pr
Elevate patients head
Inspect skin & toe nails
Medicate with nifedipine
Indications for Digital Rectal
Examination
•
•
•
•
•
•
•
•
Sensation
Tone
Outcome
Medication
Presence
Effect & Evaluation
Removal
Stimulation
Indications to perform a Manual
Removal of Faeces
•
•
•
•
•
•
Failure of other bowel techniques
Loading or impaction
Incomplete defaecation
Inability to defaecate
Neurogenic cause of bowel dysfunction
Spinal Injury patients
Consent and legal issues
Lawful Consent
• Consent should be given by
someone with the mental
ability to do so
• sufficient information should be
given to the patient
• Consent must be freely given
Considerations –
• Adults unable to give consent
• Children
Conclusion
• Health care practitioners
play a key role
• An holistic assessment is
essential
• Establish the underlying
cause and thus plan
treatment accordingly
• Patient/general
public
education on prevention
of constipation
.
Any questions?
Contact details:
alison.bardsley@continence-uk.com
With thanks to…
Norgine Pharmaceuticals Ltd. for providing an
educational grant to support this workshop.