Ramsay - CCO Oregon

Community Collaboration for
Clinical Transformation:
Designing and Implementing the TriCounty Health
Commons Grant
Rebecca Ramsay, BSN, MPH
Director – Community Care Programs, CareOregon
January 8, 2013
Setting the Stage for Broader
Transformation Efforts
• Oregon Medical Home Provider Initiatives
(2006)
– Primary Care Renewal: Managed Care / Provider collaborative;
CareOregon, OHSU Family Practice, Legacy IM Residency, Central City
Concern, Virginia Garcia, MCHD
• Major Tri County Safety Net providers involved (40% network)
• Organized as “Learning Collaborative” among partners based on a model from South Central Foundation
• 2009: PCR Payment model co designed
• Other Transformation Initiatives (2007)
– Major TriCounty Health Plan Collaboration on key initiatives
• OHLC High Value Medical Home Care Management Initiative
• OHLC Initiatives on High Tech Imaging, Early Deliveries <39wks
Just as things with CCO legislation is heating up
TriCounty “ Model of Care ” Process
• Agreement that “ changing the delivery of care ” is critical to long term sustainability
– Model of Care Ctte formed to engage providers in redesign based on their practice experience
• Charged with studying population data, then forming ideal transformative model as goal…
• Everyone wants to be at the table, has ideas
– From ctte to large advisory board
– “ Crowdsourcing
Transformation ”
Organizations contributing
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Oregon Center for Children and Youth with
Special Health Needs (OCCYSHN)
CareOregon
Legacy
Kaiser
Multnomah County
OHSU
Portland IPA
Virginia Garcia
Women’s Health Alliance
Northwest Cardiovascular Institute
Oregon Clinic
VA
Marquis
Metropolitan Pediatrics
Children’s Health Alliance
Providence
Washington County
Clackamas County
Acumentra
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Familias en Accion
Coalition of Communities of Color
Intel
Central City Concern
Coalition of Community Clinics
Cascadia Behavioral Health
Oregon College of Emergency Physicians
ODS
Family Care Health Plans
Oregon Pediatric Improvement Partnership
Alliance of Culturally Specific Behavioral
Health Providers
Lifeworks Northwest
Oregon Department of Public Health
OCHIN
Pacific Medical Group
Adventist Health
“ Tactical Groups ”
Identifying opportunities for investment
Prioritizing initiatives for implementation
1. Transitions of Care
2. High Utilizers
3. Emergency Department
4. Health Home
5. Behavioral/Physical Integration
6. Specialty Care
Timeline: Basic work done by end of March, implementation planning in April.
Delivery System Change
“ Idea Inventory ”
Up to $30 Million
Funding Over 3 Years
Application Due:
Jan 27, 2012
December 2011…
“Complete Alignment With Oregon
Challenge and Assets”
• Need to take cost out of system rapidly by improving quality, efficiency, outcomes
• Established State Leadership in Health Care Reform: from OHP to CCOs
• Established history of multi party cooperation through OHLC
• Proven safety net success in Primary Care homes: established cost reductions
• Existing projects in place that can be scaled to meet challenge…
Seed Funding for CCO Development???
TriCounty Health Commons Grant
“Transforming Health Together”
Designing the “Health Commons” Grant
Initiative
• What are the major drivers of “avoidable” cost?
• What are we currently doing to address cost that we can take to scale?
• How do we prioritize potential initiatives?
• What provides the most return with least investment
• What gives us the quickest return?
• A single organization cannot do this alone, how can we work together?
10
Very High Prevalence of Mental
Health and Addictions
(State of Oregon DMAP Data)
Mental Illness
Chemical Dependency
Attention Deficit Disorder
Post-traumatic Stress Disorder
Diabetes
Asthma/Emphysema/COPD
Heart Disease
Hepatitis C
End-stage Renal Disease
Dementia
Cancer
HIV/AIDS
11
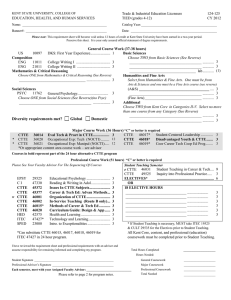
2009 Total Billed
Charges =
$1,630,851,673
Where is the $$$ going?
% of Total Billed Charges by Service
(State of Oregon Medicaid Data)
Hospitalizations and ER admits amount to 43% of Billed
Charges
* Outpatient Behavioral includes mental health services and ER and non-ER chemical dependency services
12
William
Chronic Heart Failure
History of Addiction to
IV Drugs and Alcohol
COPD
Schizoaffective
Disorder
Intermittent
Homelessness
October 2011:
Admitted to the hospital for almost a month for acute complications of his
Chronic Heart Failure. Had a previous
25 day admission 5 months earlier.
62 Year Old Caucasian Man
Developmental
Disorder
Hepatitis C
Type 2
Diabetes
13
Obvious conclusion
Even a stellar primary care home isn’t enough to meet William’s needs.
What William Needs
(to lower cost and improve health)
• Someone who is willing and has the time to deeply understand his holistic needs and health-related goals AND is accountable for coordinating needed services and teaching/coaching him (or a caregiver) in the process
• Social services such as supportive housing, daytime mental health drop-in centers, food security
• Timely, reliable access to a primary care team that knows him well, and is promptly notified and collaborated with when he accesses other parts of the health care system
• Hospital and ED care systems that can readily access information about
William’s care needs and his care team; safe transitions between sites of care
• Timely, reliable access to mental health and addiction services that follow him over time
15
TriCounty Health Commons Initiative
Improving lives for high-acuity/high-cost patients across the care continuum
Primary Care
Community Outreach
Model
Workforce: Community
Outreach Worker,
Outreach RNs, and
Outreach SW and
Recovery Mentors
Emergency
Services
• ED Navigation to
Primary Care
• EMS Community
Outreach Model
Specialty Care
Community Outreach
Model
Workforce: Community
Outreach RN and
Respiratory Therapist
Workforce: ED
Guides, Outreach
Behavioral Health
Staff
Hospital Care
Intensive Care
Transition Support
Workforce:
Transitional Care
RNS and Clinical
Pharmacists,
Transitional Care
LCSWs
Behavioral Health
Community Outreach “Peer” Model
Workforce: Peer Wellness Specialists
16
Health Commons Grant
Accountability Structure
HSO Board
Grant Oversight
Ctte
Learning System
Workgroup
Project
Management
Workgroup
Intervention
Leads/ Intersection
Group
Evaluation
Workgroup
IT Workgroup
ED Steering
Ctte
Outreach
Steering Ctte
Standard
Transitions
Steering Ctte
Hospital to Home
Transitions
Steering Ctte
Behavioral Health
Transitions
Steering Ctte
What Does Our Community Learning
System Look Like Thus Far?
• Each intervention develops its own iterative learning methods, ie case-based conferences, team-based learning retreats, site-based programmatic operations meetings, etc
• We “visit” each other’s conferences and retreats to spread ideas and insights
• Each intervention creates a dashboard of metrics with visual management systems to track ongoing progress (in development); dashboards are shared at Intersection Group
• Evaluation “swat” team (CORE at Providence) interviews patients, providers, and administrators to understand ongoing best-practice trends and common “stuck-points”; feeds qualitative information back for iterative programmatic improvement
• Community-wide learning collaboratives bimonthly
18
Learning Session #1
February 22, 2013
Collaborative Learning for
The Health Commons
Learning Session #3
June 28, 2013
Learning Session #5
October 25, 2013
Learning Session #2
April 26, 2013
Learning Session #4
August 23, 2013
Learning Session #6
December 13, 2013
19