NIHR Seminar Navigating the network
advertisement

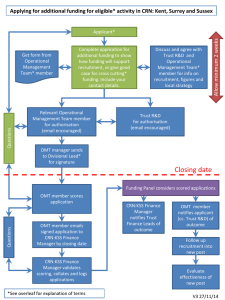
Navigating the Networks Chantal Sunter July 2014 Aims of today: 1. NIHR CRN Networks a) Then, Now & the Future b) Accessing Support 2. AcoRD Guidance & Costings 3. Questions What is the NIHR CRN NIHR Clinical Research Network (NIHR CRN) is the clinical research delivery arm of the NHS in England NHS CRN provide support to several thousand studies in the NHS every year – a large proportion of the research that takes place Journey so far… NIHR Clinical Research Network (NIHR CRN) is the clinical research delivery arm of the NHS in England Original Aims of the Networks 1 2 Increase the number of high quality studies Increase the number of participants recruited to those studies (Double in 5 years) 3 Support swift set up of studies including ID of additional sites Support recruitment into those studies by engaging clinical teams Ensure studies recruit to time and target Support PPI involvement Commercial studies 4 5 6 7 Patient Recruitment* (2013/14) *England wide • • • • Recruitment milestone This is the fourth consecutive year that the Network has surpassed its target to recruit 500,000 patients per year to clinical studies The Network has recruited more than three million patients to clinical studies in the last six years Nearly 96,000 of these patients were recruited to commercial contract studies NHS engagement • The proportion of research-active Trusts recruiting patients onto NIHR CRN Portfolio studies remains high at over 99% • The number of Trusts engaged in commercial contract clinical research is increasing year on year. 86% of Trusts now recruit patients onto NIHR CRN Portfolio commercial contract studies • Future challenge – Any Qualified Providers (AWP’s) NIHR CRN Portfolio 2013/14 England wide Study set-up 2013/14 England wide Study Delivery 2013/14 England wide Supporting Industry 2013/14 England wide Summary so far • • • • Trends show that the environment for delivery of clinical studies in the NHS in England is improving There is widespread engagement amongst healthcare providers Patient recruitment is up Study set-up times are down • The Network is not complacent – still driving performance improvements across all parts of the service • • Inconsistent geographical coverage 102 local research networks Duplication increase in hosting costs, finance, HR etc Inconsistencies in support available • Time for Change Transition is a product of our success, it is important that we change to ensure we can continue to deliver clinical research to make patients, and the NHS, better Evolution not Revolution Why Transition? Transition Programme Benefit 1 Equality of access to research for patients 2 Embedding of research into the new health and social care structures 3 Enhanced engagement within the NHS and the life-sciences sector 4 Increased efficiency through reduced transaction costs and increased productivity 5 Transparent, consistent governance and clear accountability 6 Improved flexibility and responsive research delivery 7 Improved staff retention and career development Benefits of Evolution What Will Change? Hosting Geographical coverage Resource coordination Organisational structures Where are we now? Where are we moving to? 9 NIHR CRN Network Coordinating Centres with 7 individual hosting agreements 1 NIHR CRN Coordinating Centre (incorporating clinical thematic leadership) with 1 hosting agreement 102 NIHR CRN comprehensive/local research networks with 102 individual hosting agreements with 70 hosts 15 Local NIHR CRN research networks (integrated) with 14 individual hosting agreements with 14 hosts (ie, 1 each) Inconsistent national coverage for research into key therapy areas Full national coverage for research into all key therapy areas Complex geographical configuration Simplified geographical configuration Dispersed model of workforce coordination Single model of workforce coordination, responsive to local need Dispersed and fragmented oversight of deployment of resources Strategic oversight for the deployment of resources at national / local partner level Inconsistent models of funding allocation/use Consistent models of funding allocation/use Complex organisational structure Streamlined organisational structure Inconsistent models of clinical leadership across networks Consistent model of clinical leadership across networks Partner organisations receiving multiple and confusing funding streams Partner organisations receiving single coordinated funding stream INTEGRATING THE NETWORKS • 2 x Cancer • 1 x Mental Health • 2 x Diabetes (partial coverage) • 1 x Stroke (partial coverage) • 1 x Primary Care • 1 x Medicines for Children • 1 x DeNDRoN • 1 x CLRN SPECIALTIES, THEMES & RESEARCH DELIVERY DIVISIONS: CLINICAL DIVISIONS: Division 1 2 Specialties in this division Cancer 3 Children, genetics, haematology, reproductive health and childbirth 4 Dementias and neurodegeneration (DeNDRoN), mental health, neurological disorders 5 Primary care, ageing, health services and delivery research, oral health and dentistry, public health, musculoskeletal disorders, dermatology 6 Anaesthesia/peri-operative medicine and pain management, critical care, injuries/emergencies, surgery, ENT, infectious diseases/microbiology, opthalmology, respiratory disorders, gastroenterology, hepatology Diabetes, stroke, cardiovascular disease metabolic and endocrine disorders, renal disorders Management & Leadership Structure Clinical Director (Dr Stephen Falk) Chief Operating Officer (Dr Mary Perkins) Nurse Consultant (Dr Sue Taylor) Senior Research Delivery Manager – Cross Cutting (Martine Cross) Industry Operations Manager (Acting - Holly Valance) LCRN Research Delivery Cross – Cutting Team Senior Research Delivery Manager: (Maxine Taylor, Div 1&3) Research Delivery Manager (TBA - Div 2&4) Research Delivery Manager (Chantal Sunter, Div 4&5) Research Delivery Divisions: Operational delivery of the LCRN portfolio managed through six nationally determined research delivery divisions, each encompassing a number of specialties Managed by a Research Delivery Manager, each Manager will form national networks of operational expertise, led nationally by a Research Delivery Director for the Division LCRN Research Delivery Managers will report to the LCRN Chief Operating Officer and be responsible for the delivery of NIHR CRN portfolio studies LCRN Support Team: The LCRN will have a Support Team to manage local operational arrangements. This team will be required to support and deliver the following functions and systems: Support functions including (some of these functions may be encompassed within research delivery roles): LCRN administration Information management Workforce development Communications Patient carer and public involvement and engagement Finance CRN systems, including information systems (for example, the CSP Module for NHS Permissions, CPMS and LPMS) Research Delivery Cross-Divisional Team Research Delivery Cross-Divisional Team will undertake delivery activities that support all clinical specialties. Activities will include the provision of: A LCRN research advice service A single point of contact service for Life Sciences Industry A Lead LCRN service and Coordinated Network Support service, in-line with national standards The NIHR Coordinated system for gaining NHS Permission (CSP) Coordination of the Research Passport Scheme What is staying the same? • Evolution not revolution • Delivery staff (Research Nurses, Clinical Studies Officers) • Fewer issues around crossing boundaries e.g. mental health staff working in primary care settings or AHP’s on mental health related studies • Contact your relevant RDM or usual Lead Research Nurse / Senior CSO if looking for study support • RDM’s working closely with R&D offices across the region • Involve the network at early stage as possible Patient and Public Involvement • • • • • PPI / PI / PCPIE / Service User Involvement Cross organisation approach and team Retaining specialty groups where appropriate ClahrcWest / WEAHSN / CRN WE / HPU Strategy group: 8 public members (2 sit on each organisation) 4 organisational members • Develop and agree strategies on common issues e.g. payment PPI (Division 4) • Currently still a dedicated PPI worker 0.4wte • Some initiatives looking to roll out across specialties: Pre-ethics materials review service Exit questionnaire Everyone Included AcoRD • Attribution of COsts of Research & Development • Formerly known as ARCO Major aim to • Improve the consistency of cost attribution • Encourage more consistent funding of the costs of research (Research Costs, Excess Treatment Costs, Service Support Costs) Major Changes • Guidance aims to clarify / correctly attribute R&D costs to either ETC, SSC or research costs • ARCO classified on the basis of WHO was carrying out the activity • AcoRD classifies on the basis of the PRIMARY PURPOSE of the activity. • Pilot of a new Costing template ACAT (Activity Capture Attribution Template) for use with full grant applications • Taking consent is classified as SSC not research cost • 2 different categories of research costs (Depends on funder) AcoRD continued Network Delivery Funding is Service Support Costs = early engagement important Currently will primarily impact AMRC funders (even when only part of the grant funding is from AMRC) Full application stage will require ACAT completion with the application (funders will inform applicants if / when required) Likely to be rolled out to all funders eventually ACAT support • AcoRD Specialists in each Clinical Research Network • You will be informed if you are required to complete the ACAT and who your local specialists are. • They will provide support in completing the ACAT (but wont complete it for you) • The completed ACAT will then be reviewed by additional ACAT reviewers following submission to funder • • Suite of support materials available at http://www.crn.nihr.ac.uk/can-help/funders-academics/support-for-noncommercial-studies/acord/ Thank you for listening Questions? Chantal.sunter@nihr.ac.uk