Presentation Title - Global Health Mini
advertisement

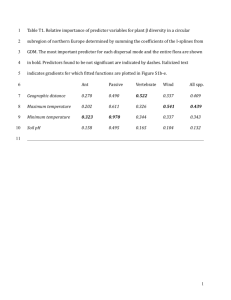
My Story Meet Tausi Suedi… AND her beautiful children! 1 Not So Good to be So Sweet: Pregnancy & Diabetes Tausi Suedi, MPH Mychelle Farmer, MD Chandrakant Ruparelia, MD,MPH Leah Hart, MSN, MPH March 7, 2014 Objectives Describe the global burden of NCDs Define gestational diabetes List adverse maternal and newborn outcomes associated with GDM Describe GDM screening and diagnosis approaches Evaluate community based innovative model for screening, diagnosis and management of GDM 3 Global Burden of Disease 65% of all deaths each year due to NCDs NCDs leading cause of death globally for women CAUSE % Cardiovascular 33.2 Infections 13.9 Cancer 13.0 Chronic Respiratory Dis. 7.3 Respiratory Infxn, TB 6.6 Injuries 5.1 OB, Perinatal 5.0 GI 3.1 Diabetes 2.6 Neuro-psychiatric 2.3 World Health Organization, 2008 Global Burden of Diabetes Zimmet PZ, Medicographia, 2011 5 50% of diabetics are undiagnosed Nearly 70% of diabetics in Africa 57% diabetics in Western Pacific Zimmet PZ, Medicographia, 2011 6 Diabetes Mellitus It is a disease in which human body either does not produce or properly use insulin that regulates blood sugar resulting in increased blood glucose. There are two type of diabetes mellitus: Type 1 and Type 2 7 Types of Diabetes Mellitus Type 1 Low or absent endogenous insulin due to beta cell damage Onset before 30 years Exogenous insulin required for life Causes: Genetic, infection Type 2 Insulin level is normal, elevated or absent insulin resistance, tissue sensitivity, & impaired beta cell function Exogenous insulin may be required for management Causes: family history, lifestyle, obesity and aging 8 Understanding the Mechanism : Insulin, Closed Glucose Transporter, Glucose, Insulin Receptor Open Glucose Transporter, 9 Gestational Diabetes Mellitus (GDM) Gestational Diabetes Mellitus (GDM) is defined as carbohydrate intolerance with recognition or onset during pregnancy’ irrespective of the treatment with diet or insulin. 10 Slide: Courtesy of Professor Peter Damm Normal Pregnancy Insulin secretion Blood glucose Insulin resistance Gestational DM Insulin secretion Insulin resistance GDM short-term outcomes Babies Macrosomia Birth trauma such as shoulder dystocia Stillbirth Neonatal hypoglycemia Mothers Birth trauma Increased rate of C-section Increased risk for post-partum hemorrhage and other causes of maternal deaths 12 GDM out long-term outcomes Babies Type 2 diabetes (33% increased risk) Mothers Type 2 diabetes (35-60% increased risk) 13 GDM and Type 2 Diabetes http://www.thenews.com.pk/article-17375-Deaths-up-from-non-communicable-diseases http://www.thehindu.com/sci-tech/health/medicine-andresearch/novel-study-in-tn-to-know-gestational-diabeteseffects/article2970820.ece 14 Recommended Practices IADPSG Diagnostic Guidelines Based on Hyperglycemia and Adverse Pregnancy Outcomes (HAPO) study Fasting glucose ≥ 5.1 mmol/L (92 mg/dl), 2 h 75 g OGTT in pregnancy One hour result of ≥ 10.0 mmol/L (180 mg/dl), Two hour result of ≥ 8.5 mmol/L (153 mg/dl). Country Case Study: India 1. Prevalence of GDM in India 2. Purpose of Jhpiego’s assessment in two Indian states 3. Results 4. Proposed community-based approach to screening 16 GDM Prevalence in India 20 18 16 17.8 % Prevalence 14 12 13.9 10 13.8 8 9.9 6 4 2 0 Urban Semi-urban Rural V.Seshiah , V. Balaji , Madhuri S Balaji.A Paneerselvam, T Arthi, M Thamizharasi, Manjula Datta , (2008). Prevalence of GDM in Asian Indians- A community-based study. JAPI , Vol 56 , pp. 329-323. Average 17 Purpose of India assessment To describe the current situation related to screening, diagnosis and management of diabetes in pregnancy at various health facility levels in the peri-urban regions of Mumbai, Maharashtra and Chennai, Tamil Nadu. http://www.mapsofindia.com/images2/india-map.jpg 18 Results of situational analysis Inconsistent use of GDM guidelines Urine dipstick testing at sub-center levels with referral Resource intensive follow up to positive urine screen Inconsistent documentation of referral results and birth complications related to GDM 19 Challenges of Clinic-based GDM Screening High volume of referral based on urine dipstick screen Fasting required High clinic volume due to 2-hour wait Up to 30% “no show” 20 Community-based GDM Screening Approach Begins at the doorstep of the pregnant woman Cost-effective and integrated in existing services Reduces healthcare facility burden while increasing detection 21 Beyond diagnosis… a public health approach Pregnant Woman in the Community --- + 12-16 weeks first ANC visit: 1st GDM Screening Screening using Glucose Challenge Test (GCT)* - Referred for diagnostic test and medical management - Meal plan and 98%! medication management - Community-based glucose monitoring - Birth preparedness and complication readiness 24-28 weeks: 2nd GDM Screening 22 Summary It is time to address GDM globally Community-based single test approach to screening for GDM is the way to go No linkages for referral? Program will fail. Improved health outcomes is the goal, with 98% of cases managed through healthy meals and lifestyle 23 Thank You! Mychelle Farmer, MD Mychelle.farmer@jhpiego.org Tausi Suedi Tausi.suedi@jhpiego.org Chandrakant Ruparelia, MD MPH Chandrakant.ruparelia@jhpiego.org Leah Hart, MSN MPH Leah.hart@jhpiego.org 24 Thank you! Please fill out an evaluation by going to this session’s page on your mobile app OR by filling out a paper evaluation in the back of the room. The Closing Session will begin at 4pm in the Grand Ballroom. Closing remarks will be followed by a 30-minute social gathering (refreshments will be served). Come meet new people and discuss the highlights of the day!